The Man Who Can Predict How Long You Have Left To Live (To The Nearest Month): Gary Brecka | E225
Now Playing
The Man Who Can Predict How Long You Have Left To Live (To The Nearest Month): Gary Brecka | E225
Transcript
2892 segments
If you want to strip fat off your body,
there is nothing, no type of
cardiovascular or weight training that
comes anywhere close to
He's spent 20 years working in life
insurance, predicting when people were
going to die to the nearest month. And
now he's on a mission to extend your
life.
Most people, they're walking around
right now at about 55% of their true
state of normal. There is an element
missing from their body that would make
the difference between them being an
average person and being a superhuman.
How? Everything that we put into our
bodies gets converted into a usable
form. If you cannot make this
conversion, you have a deficiency. And
it is this deficiency that leads to
these conditions.
They have accepted something as either a
consequence of aging, stress, or their
environment. This not a consequence of
any of those things. I'm going to tell
you exactly how to find out what it is
that's missing, so you could thrive in a
way that you probably never thought
possible. Let's use Dana White as an
example. So, LabCorp calls us, so says,
"Hey, we have a life-threatening alert
on a patient." He had all of these
conditions.
I've been talking to doctors. None of
them could fix any of my problems. I
said, "I'm surprised you could even
sleep through the night without choking,
gagging." He's like, slammed his hand
down, "How did you know that?" And I
said, "If you don't do what we're going
to ask you to do, if you have a life
expectancy of 10.4 years." And in 10
weeks, he has such a material change,
and he was like, "I had no idea I could
feel this good."
And his life expectancy? Almost tripled.
Someone who's just heard that at home,
where do they start? So,
I just want to start this episode with a
message of thanks. A thank you to
everybody that tunes in to listen to
this podcast. By doing so, you've
enabled me to live out my dream, but
also for many members of our team to
live out their dreams, too. It's one of
the greatest privileges I could never
have dreamed of or imagined in my life
to get to do this, to get to learn from
these people, to get to have these
conversations, to get to interrogate
them from a very selfish perspective,
trying to solve problems I have in my
life. So, I feel like I owe you a huge
thank you for being here and for
listening to these episodes and for
making this platform what it is. Can I
ask you a favor?
I can't tell you how much um you can
change the course of this podcast, the
the the course of the guests we're able
to invite to the show, and to the course
of everything that we do here just by
doing one simple thing. And that simple
thing is hitting that subscribe button.
Helps this channel more than I could
ever explain. The guests on this
platform are incredible because so many
of you have hit that button and I know
when we think about what we want to do
together over the next year on this
show, a lot of it is going to be fueled
by the amount of you that are subscribed
and that tune into this show every week.
So, thank you. Let's keep doing this and
I can't wait to see what this year
brings for this show, for us as a
community, and for this platform.
Gary. Yes.
I This is the first time I've started
this podcast in this particular way, but
I was
but this is where I wanted to start it.
It's with a slightly curious question,
which is
there's people that have just clicked
onto this podcast to listen now, right?
YouTube, Spotify, Apple, wherever
they're listening.
Um
why should they
stay and listen to the message that you
have committed your life to spreading?
Because
everybody wants to be better, right? I
mean, everybody wants to improve their
health. And most people, especially
young people,
probably don't realize that they're
walking around right now at about 55%,
maybe 60% of their true state of normal.
There is
a nutrient, an amino acid, a substrate,
a compound, um
an element missing from their body
that if they knew what it was
would make the difference between them
being an average person and being a
superhuman. They have accepted something
as either a consequence of aging or a
consequence of stress or a consequence
of their environment, something like
brain fog, or repeated poor sleep, or
weight gain, or water retention, or not
the healthiest response to exercise, or
brain fog, or poor short-term recall, or
any number of things that they've
accepted as consequence of life, of
aging, of stress, or what have you,
it's not a consequence of any of those
things.
It's a consequence of missing raw
material.
And I'm going to describe that in detail
and tell you exactly how to put that raw
material back into your body,
and how to find out what it is that's
missing,
so you could thrive in a way that you
probably never thought possible. Who are
you? Um I'm a human biologist,
um and a researcher, biohacker. My
background is in
uh of all things mortality science. You
know, my undergraduate degrees were in
biology, my postgraduate degrees are in
human biology. I'm fascinated by the
human body, um its form, its function,
how we can improve its performance, and
I'm a researcher. You know, I spent 22
years um
as a mortality expert in the insurance
industry,
which meant that if we got 5 years of
demographic data on you, and 5 years of
medical records, we could tell the
insurance company how long you had to
live to the month. To the month? To the
month. And I get a lot of flak about
that. People say, "Oh, if you could
predict death to the month, you'd win a
Nobel Prize, or you know, only God can
tell you when you're going to die." I
mean, and that's very true. I mean,
obviously, if we do a mortality
prediction on you, it doesn't mean
December 12th, you know, 2065, you're
going to drop dead on that day.
But it is very accurate science. You
know, if you think of the most
successful financial institutions on the
planet as a category, are insurance
companies.
If you look at the failures during the
2008-2009 financial crisis, which was a
global crisis, you know, in the US, we
had 364 banks fail. You didn't have a
single life insurance company fail. No
other financial institution, no other
investment enterprise, hedge fund, angel
investor, um venture capital firm would
ever put tens of millions of dollars at
risk
on any kind of investment on one single
variable.
Yet every time a life insurance company
bets on your life or or issues an
annuity or a reverse mortgage or any
number of other financial services
instruments that are based on mortality,
they're only betting on one factor. They
don't care where you are on a mortality
curve. They want to know how many more
months does this person have left on
Earth? And they needed some of the most
accurate science on the planet.
And
they have perfected this and the good
news is
that this science is very accurate and
I'm going to share a lot of the details
of that today, but
the downside of this industry and the
reason why I left it was that
during my tenure in this career
I was not allowed to have any contact
with the patient or any contact with the
treating physician. Now, I'm not
licensed to practice medicine. I'm a
human biologist.
But if I was reading a medical record
and saw a life-threatening drug
interaction, I could not contact the
patient.
And this database where this information
is drawn from, if this database could
see the light of day
I believe it would permanently change
the face of humanity. It would upend
modern medicine in a way that would be
completely catastrophic because you see
they have information that no other
database has, no other research study,
no other you know, financial
institution, no other
university has and that is that they
know the day, the date, the time, the
location, and the cause of death for
hundreds of millions of people that they
have all of these records on.
You know, if I if I'm a cardiologist and
you come in to see me and I put a heart
stent in your heart. Well, when you
leave my office, I don't know what
happens to you two months later, two
years later, 12 years later. I don't
know if you died as a consequence of
something that went wrong with the
procedure I did or if you died of
something completely different. I don't
know exactly what kind of impact on your
life that procedure had or didn't have
Um, unless it's contained in a very
short-term clinical study.
And
uh, not that I want to go into the whole
science of mortality, but
if you had access to this database, you
would realize that the most common
ailments that we suffer from
are not diseases and pathology that are
happening to us. They are things that
are happening within us.
You know, I always say that if I was to
boil my entire career down to a single
sentence, it would be
that the presence of oxygen is the
absence of disease.
And nothing is more impactful than that
statement.
The presence of oxygen is the absence of
disease. I have yet to find a single
disease etiological pathway, something
that's happening in in the human body
causing pathology, causing disease,
dysfunction, that doesn't have its roots
in a lack of blood oxygen or its roots
is not aggravated by something called
hypoxia, lack of oxygen. In fact, all
human beings die of the same thing. We
all leave this earth the same way.
Right? We all die of hypoxia, lack of
oxygen to the brain. That's the
definition of death. Only we tend to
think of it as an event. Right? A
gunshot wound, a bus, car, a stroke,
heart attack. But the truth is, we are
on a hypoxic curve.
Meaning we are accelerating quickly or
accelerating slowly towards the grave.
And the second thing that we discovered
in this
um, voluminous data-driven industry
was that
when you deplete certain raw materials
in the human body,
you get the expression of that
deficiency. So, what I mean is, you
know, we've all heard that um,
uh, disease, you know, travels in
families or you might have genetically
inherited hypertension or genetically
inherited hypothyroid, genetically
inherited drug and alcohol addiction,
diabetes, um, depression, anxiety. These
things tend to run in families. So,
we've accepted the myth in most cases
that these are genetically inherited
diseases.
But think about this, the next time one
of your listeners gets told that, "Oh,
you have genetically inherited
hypertension." What we call uh
idiopathic hypertension, or genetically
inherited hypothyroid, or if you have
this genetically inherited disease, or
that genetically inherited disease. Stop
your physician and say, "Well,
wait a minute. We We've mapped the
entire human genome.
Um so, we know every gene in the human
body. Can you tell me what disease I
inherited from my ancestor that's
actually causing this condition?"
And watch their face go blank.
Because in the majority of cases, we
have accepted that disease travels in
families when it's actually not the
disease being passed from generation to
generation. It is the inability for
their body to refine a certain raw
material,
which causes a deficiency,
which leads to that disease.
So, in other words, there's not a single
compound known to mankind, not one,
no mineral, vitamin, amino acid,
protein, carbohydrate, no nutrient of
any kind, no element known to man, that
enters the human body
and is used in the format that we put it
in. Everything that we put into our
bodies gets taken in by the body and
converted into the usable form.
If you cannot make this conversion,
you have a deficiency.
And it is this deficiency
that leads to these conditions.
And so, if you go hunting for that
deficiency and you supplement, not for
the sake of supplementing, but you
supplement for the sake of deficiency,
magic things happen in human beings.
There is a superhuman inside of every
person listening to this podcast, and if
they actually were able to test
themselves to a genetic test and look at
what's called their methylation, how
their body refines raw materials, and
they were able to replace the deficiency
that is holding their body back from
creating adequate levels of
neurotransmitter and achieving normal
new mood, moving um
contents through the gut and achieving
normal gut function,
um elevating emotional state, deepening
their sleep, quieting their mind. All of
these conditions that society has
labeled different pathologies and
disease.
Uh
then they would begin to thrive in a way
that they just never thought possible.
It's so blatantly clear how passionate
you are about the subject matter, which
begs the question. You know, I remember
when I was reading through
your story
I I uncovered that you'd read
hundreds of peer-reviewed papers. I
think the quote was something along the
lines of Um if there's a peer-reviewed
paper on the subject matter of
biohacking and um disease and longevity
and those kinds of things, you've
basically read it. So this begs the
question to me, like why is one
individual so unbelievably passionate
about this subject matter? And
I would like you to take me as early as
you possibly can to answer that question
in your own life. Where did your
obsession, passion, where was it
fostered fostered and nurtured so that
you spent and committed your life to
this subject matter? Where did that
begin? So it actually began I I grew up
on a
very large tobacco farm. My my father
was a Navy captain, my mom was a flight
attendant, she worked for the airlines.
But we had a
a farm that we leased out to other
farmers. And surrounding this 300-acre
tobacco farm were all kinds of animal
farms. There were cattle farms, there
were chicken farms, there were
horse farms.
And I was an only child. My nearest
neighbor was miles away. In fact, from
my home you couldn't even see another
house from my parents' house until I was
in my early 20s.
And so for me to to play with another
child, I had to get on a bike and spend
half an afternoon biking to their house.
So I got very familiar with the farm and
I was always just fascinated
by the veterinarians that would come
onto these farms and fix horses and fix
cattle and fix sheep and fix chickens.
And I always thought it was so cool that
these animals could be laying on the
ground seemingly about to die and the
veterinarian would come come on board
and do a bunch of stuff and the next
thing you know this horse was up and a
few days later it was galloping back in
the field or
um you had
all kinds of strange things that would
happen on this farm and there was always
someone arriving to just fix it and I
started to get fascinated with medicine
I guess in that way. I always found it
as a way to take something that was sick
and helpless and sort of help it get
back to normal function.
And I found out in the eighth grade uh
sometime during my eighth grade year
that uh I was clinically photographic.
So I have a clinical level of
photographic recall which is different
than just having a
uh visual memory. I'm I'm clinically
photographic so I have a voluminous
capacity to recall things that I read
even if I don't understand them which is
why I never read for pleasure. Um I'm
very cautious about what I read and very
cautious about what I look at
um because I record everything. So I
can't be flying on American Airlines and
take the seat back magazine out and read
the seat back magazine because
3 months later I'll tell you where the
sales center is for a
condo project in Buenos Aires. You know
it's so I can I can fill my brain with
senseless things like that and record it
and regurgitate it um or I can fill it
full of things that that fascinate me
and so I naturally gravitated towards
science. Is that what they call a
photograph photographic memory?
Photographic memory is usually someone
that can remember seven numbers in
sequence. They have extremely good
recall for things that they visualize.
Clinically photographic is being able to
regurgitate voluminous amounts of
information with incredible accuracy. So
I still remember
you know section 15.2 sub paragraph B of
my first employment contract that I
signed 28 years ago.
Really?
Really? Yeah. I remember I remember
that. It was actually with a trading
firm
um that I signed it with so
you know when I read peer reviewed
papers um in scientific journals, uh it
doesn't make me more intelligent than
someone because very often I can recall
information that I don't understand. So,
I can regurgitate voluminous amounts of
information. So, subjects that rely on
rote memorization like chemistry,
biology, neurobiology, microbiology, a
lot of these sciences don't actually
make sense.
Right? That you just have to memorize
how they operate. Chemistry in a lot of
ways doesn't make sense. Right? Um you
just have to remember what happens when
you put these two elements together,
they create this. So, you know, when you
pull a carbon bond or you double a
carbon bond here or hydrogen bond there
that you you that the molecule shifts in
this way.
And so, I gravitated towards science. I
got my undergraduate degree in biology.
How did you do? Um I did very well. I
actually found it quite the breeze. Um
my you know, when I was an undergrad, my
you know, biology, chemistry were
considered the toughest majors. And I
went to branch campus University of
Maryland. A lot of my roommates were
political science, not investing on
political science majors at all, or
philosophy, or psychology, and they got
to party all the time, and you know, I
had
really intense classes, you know,
morphology of thallophytes and chemistry
and and you know, biomechanics and and
science and
and a lot of plant biology courses and
human biology courses.
But I was able to have the same kind of
social life that they were because I
would, you know, record a lecture and
then I would regurgitate the lecture
when I needed it during during a test.
Is it a gift or a curse? Because with
all things in life that appear to be
gifts, there's often some kind of hidden
curse. Well, the curse is that I can't I
I rarely read for pleasure. Um it's very
difficult to read for pleasure because I
record all of that information. So, when
I'm going in to read a book, you know, a
lot of people
read a book that they didn't really
like,
it doesn't stay with them. Um or they
read a fiction novel, it doesn't really
give them any benefit. It's not doesn't
doesn't feed them, but they do it to
relax or they do it for entertainment.
For me, it would take up storage.
I would record that information. So,
there's no need for me to have that
information in my possession. I find
other ways to
to relax and
and and meditate and unwind, but reading
for pleasure is just just not one of
them. So, I guess that could be a curse.
But, you know, then I went to grad
school for human biology. I went to
another 4 years of school for human
biology. So, I had 8 years of science.
And then I was um
either going to go into chiropractic or
into orthopedic medicine. I really like
the idea of orthopedics because again,
an orthopedic surgeon was somebody that
fixed people. And
you know, an internist was somebody that
just managed disease. You know, they
took a
obese hypertensive diabetic uh patient
and they just kind of managed their case
throughout their lifetime, but I felt
like an orthopedic was somebody that you
know, you came in and you had a broken
leg and
they
you know, fixed your broken leg and and
you were back to normal. I like the idea
of fixing things and and kind of
returning function back to people. And I
took some time off, uh you know, after I
got my human biology degree and I ended
up going into
a rare area of science, um this
mortality science,
um
for life insurance and secondary life
insurance
where you would take medical records and
demographic data and you would use this
in what's called a probabilistic model
to predict life expectancy.
And I was fascinated by it cuz I loved
the big data nature of it. And for years
I actually subscribed to the fact that
this was just data.
And
that
I had no influence on this person's
outcome. I didn't put them in this
position nor am I responsible for
getting them out of this position.
But, eventually I think as both my faith
grew and my awareness of the fact that
there were human beings on the other
side of these spreadsheets,
I finally made a conscious decision to
say, "What am I doing? I'm going to
spend the rest of my life just
predicting death um for the monetary
gain
of an investor
versus taking this information and
helping people live healthier, happier,
longer, more fulfilling lives. Because
by studying medical records and you
know, I read you know,
8 to 10 hours a day, 6 days a week,
thousands and thousands and thousands of
medical records and extracted from those
how we would impact somebody's outcome
of their life, you know, how how it
would impact the length of or the the
shortness of the duration of their life,
their health span or their lifespan.
And once you realize there's human
beings on the other side of the
spreadsheet, you start to feel like
you're sitting behind a thick glass wall
just watching blind people walk into
traffic.
And
towards the tail end I used to
artificially kind of manipulate the
record. I would say, "Well, what if I
what if I artificially fixed this
person's D3 deficiency? What if I cured
the anemia? What if I actually
um noticed that they had a gene mutation
called MTHFR instead of trying to fix
them with folic acid, I fixed them with
methylfolate?" And you would just see
the life expectancy jump. In the model?
In the model. Yeah. Right. And this
model was based on very large data. So,
it was very likely to have a real life
impact. And when I say we predicted
death to the month, it was based on that
patient's current position. And doesn't
mean that they couldn't walk out the the
next day and and and get hit by a bus or
or die in a commercial airline, you
know, disaster or something like that.
But there's there were standard
deviations that would account for those
kinds of risks. What the insurance
company wanted to quantify or the
annuity company or the reverse mortgage
company wanted to quantify was based on
this person's everything that we know
about this person right now, the
function of their liver, the slightly
hypoxic anemic profile that they have,
the deficiencies that they have in
vitamin D3, the suppressed immune
system,
um you know, the elevated visceral fat,
the body mass index, the bone mineral
density. Based on all of these things,
when do these things all meet and
actually cause a catastrophic event
catastrophic event? And there were
things called mortality debits and
comorbidity debits and you know, we put
all these together and I really like the
data of it. But realizing that there
were human beings on the other side of
the spreadsheet just woke me up and I
said, you know, I have this
chasm of knowledge. Even though I'm not
a physician,
I have a fundamental understanding of
human physiology. I'm fascinated by
human physiology and ways that we can
improve um lifespan and health span.
And so why wouldn't I take this
gift and get into an industry
like wellness or functional medicine
where I could actually make a
difference. Where instead of predicting
death, we could extend life. And in
doing so, help people live healthier,
happier, longer lives, more fulfilling
lives, get rid of a lot of the ailments
that people suffer from. I mean, when
you when you start to peel back the way
that modern medicine defines a lot of
conditions that we have, you know, take
um depression or anxiety or ADD or ADHD
because a lot of your listeners are
probably entrepreneurs. And a lot of
entrepreneurs have very active minds and
they've been told they have attention
deficit disorder, right? Or attention
deficit hyperactivity disorder. Well,
attention deficit disorder is not an
attention deficit at all.
Um we misdefine these things. It's an
attention overload disorder because you
see in the human brain, we don't just
create thought.
We also dismantle thought. It is just as
important for you to be able to create a
new thought or feeling as it is to
dismantle it. Right? And if you don't
degrade thought called catecholamines,
if you don't degrade them, then there's
a gene that governs this,
catechol-O-methyltransferase.
If you create thought at a faster rate
than you degrade thought, then the mind
gets very clouded. And so, attention
deficit disorder is attention overload
disorder. It's too many windows open at
the same time.
So, modern medicine says, "Well, if the
mind's racing, let's put an amphetamine
into the body, race the central nervous
system to match the pace of the mind."
And this is a very poor choice, right?
Because eventually this will burn you
out. Can actually change the
neuroplasticity of the brain. Rather
than put the right amino acids back into
the body, the right complex blend, um
the right methylated folates, so that
the mind can actually begin to quiet.
What would you say to someone that says
that ADHD is also in some ways a result
of some early trauma?
Well, you know, trauma's always
fascinating to me. Trauma can trigger
methylation. Trauma can interrupt the
methylation cycle.
Right? But the the idea in modern
medicine that you have some kind of
trauma, you have a disrupted
relationship with your
mother, for example, and that somehow
we're going to go and put
neuroplasticity altering chemicals into
the brain, and it's going to fix this
30-year broken relationship you have
with your mother. To me,
it doesn't Yeah, yeah, yeah. make any
sense, right? And so, it's not at all to
poopoo trauma, to to to put trauma down.
Depression really exists, anxiety really
exists, but but if you actually look at
how we define these conditions, take
depression, for example. We define
depression, at least in America, we
define depression as an inadequate
supply of serotonin.
Right? So, if you're a low in serotonin,
you're by definition depressed. So, then
you would think that the solution would
be to raise serotonin.
Right? If we define depression as low
serotonin, you'd think that the solution
would be to raise serotonin, but that's
not what we do. We take people that are
depressed and we put them on SSRIs,
selective serotonin reuptake inhibitors.
And what these do is they ration what
little serotonin these people have.
So, by definition, it never raises
serotonin. So, by definition, it never
ends depression. I mean, I have I have
clients come in to see me all the time,
and and and and our clinical team and
then I'll say, "Well, how long have you
been on antidepressants?" They say, "15
years, 18 years." And my first question
is, "Well, when did you think it was
going to kick in?"
Right? So, if we understand that
serotonin is actually methylated in the
gut, this process that I'm talking about
is called methylation. We actually make
serotonin from an amino acid called
tryptophan, the one that's famous for
making you sleepy after Thanksgiving
dinner. I know you guys don't have
Thanksgiving in the UK, but I'm from
America, but um so, you guys we eat a
lot of turkey on Thanksgiving and turkey
has a lot of tryptophan. So, when you
take um tryptophan methylate it into the
neurotransmitter serotonin, of which 90%
resides in your gut.
Methylate is basically processing.
Yeah, the processing. It's like the
refining process. Crude oil gets refined
into gasoline.
Amino acids get methylated into
neurotransmitters. Okay. And so, this
process of methylation
when it's broken and and it can be
relatively easy to fix. When it's broken
it means that we have an impaired
ability to create. We have an impaired
ability to um refine a raw material and
it leads to this deficit. Well,
serotonin for example, 90% of it resides
in your gut. So, if you don't have it
here, you can't have it here. So,
depression rarely begins in the outside
environment. It usually begins in the
gut. Now, it may be trauma that led to
the deficiency.
But, the fix is not in a chemical or
synthetic or pharmaceutical blocking the
brain's capacity to uptake these
neurotransmitters. The fix is in
restoring adequate levels to the body so
it can naturopathically make its way
back up the vagus nerve and and arrive
to the brain. Sim- similar things are
true with anxiety. I mean, if you
actually have ever suffered from or know
somebody who's suffered from anxiety, if
you ask them three questions, you can
find out very quickly that their anxiety
is not coming from a cluster of
symptoms. It's not coming from their
outside environment. It is coming from
within them. It's coming from their
physiology.
Right? I mean, if you know someone who's
suffering from anxiety and you say well
have you had anxiety on and off
throughout your lifetime?
The most of the time they'll say yes.
And then if you say can you point to the
specific trigger that causes it?
Very often they'll say no.
I mean yes I know some of my triggers
but I could be sitting in a podcast just
like this in a very calm environment
there's no threats around and all of a
sudden I get overwhelmed by anxiety. I
can be driving home from work on an
otherwise innocuous day and I can be
overwhelmed by anxiety. Well that is not
coming from your outside environment.
Right? This is coming from a process
called methylation and it is caused from
excess catecholamines entering the brain
and an inability to down regulate these.
So the body's entering this mild fight
or flight response without the presence
of a fear.
See remember that as sophisticated as we
like to think our brains are it's really
not. Our brain is very primal.
You know what the brain cares about? The
brain cares about survival.
And so doesn't care how fat or skinny
you are how pretty or
ugly you are it doesn't care about your
skin your hair it cares about survival.
And so when we understand that the brain
does not know the difference between
perception and reality
we start to understand how it can play
tricks on us. So I always use the
example that let's say you drove home
tonight
and you got out of your car when you got
home you got out of your car and
somebody was standing in front of you
with a knife.
It's a very real threat. Right? You'd
have a fight or flight response. Your
pupils would dilate your heart rate
would increase your extremities would
flood with blood your hearing would get
very acute your brain would flood with
catecholamines you're getting ready to
fight or flight.
But you could also be laying on the 30th
floor of a condo building in bed and
start thinking about getting eaten by a
shark.
There is zero chance of a shark getting
out of the ocean going up a 30th floor
elevator. Right? Coming into your condo
and biting you in that bed but you can
have the exact same response.
If you're watching a movie or something.
Exactly. So one is entirely real one is
entirely perceived. The physiological
response is identical.
So now once we understand this, now we
begin to understand how I can feel the
presence of a fear, which is what
anxiety is. It's a fear of something
happening in the future. Usually it's
not going to happen. Usually hasn't
happened in the past and is not likely
to happen. But it's it's this fear
starts to build up. You start to get
very anxious. It can actually change
your heart rate um to the point where
you can panic attacks can land you in
the hospital.
Um or it can be mild enough that it just
causes you anxiousness. Mild anxiety.
But there's no presence of a fear. And
so you start trying to correlate it to
your outside environment. Starts to
drive you crazy because you go, "Well, I
don't get it. I'm on vacation with my
wife and or my spouse and my kids and
I'm in the resort of a lifetime. I've
been here a thousand times. I love this
place. There's no reason I should feel
like this." But all of a sudden you have
this feeling of anxiousness, anxiety. So
these are these are lack of raw material
in the human body. My mission is to try
to help people by taking a genetic test
um once in their lifetime, find out
where is methylation broken, and then
stop supplementing just for the sake of
supplementing, and start supplementing
for this deficiency so your body can
thrive. In the case of people that are
listening to this now and they can
pinpoint the moments where they've
gotten anxiety. So say they've I
remember I had one guest on the podcast
maybe two years ago
and after he became famous, he developed
social anxiety.
Mhm. So he whenever he would be with
around a lot of people, he'd feel that
sense of anxiety. And then from that
sort of capitalistic moment, then when
he's at home, he'd get the same rush of
anxiety, but he would point to that
capitalistic moment of becoming famous,
and then some things had happened in his
life, and then he'd get anxiety at home
when nothing was going on. Right.
In that situation, what's the the
nutrient
you go. So so now you've you've you've
interrupted methylation because there is
one where there is the presence of fear
and there's one where there isn't. Yeah,
there's the absence of a fear. So to be
very specific, anxiety, true anxiety
does exist, but you can point to the
specific trigger that causes it. So, for
example, if you if you have a fear of
heights and you walk to the edge of a
30th floor balcony and look over it,
you're going to feel anxiety. If you're
claustrophobic and you step on a really
crowded elevator, you're going to feel
anxiety. But, if you're claustrophobic
and you're sitting at home
and you start to become overwhelmed with
anxiety, this is actually not coming
from that trigger. This is coming from
your physiology. And the way that we
deal with stress, right? And like
cortisol, when you measure cortisol
levels, cortisol's not really a measure
of how much stress is in your life, it's
a measure of your body's reaction to
stress. So, why are some people more
resilient to stress and don't have
anxiety attacks and why are other people
not as resistant? Again, this is not to
say that if you didn't have
a violent attack in your life or or a
terrible car accident that sometimes
when you've had a
you know, a a vehicle accident and you
approach an intersection,
the the the
the memory of having been T-boned, you
know, recently and badly injured is
going to give you anxiety. But, the
majority of people are not suffering
from that type of hyper-specific
situational anxiety. They're suffering
from something called generalized
anxiety or idiopathic anxiety, which
means of unknown origin. So, for
somebody who's very famous and gets into
a a crowd and doesn't know who's coming
at them, that's a very I wouldn't even
define that as anxiety. That's a very
primal instinctual reaction to a real
fear. Mhm. Right? Just like walking to
the edge of a 30th floor balcony. What's
not a primal reaction to a real fear is
when there is no presence of a fear,
especially if that incident has never
happened and you aren't even sure what
you are afraid of or why you are anxious
or why you have anxiety, then this is
coming from your physiology. So, how
would you treat that? You look at the
different There are five major
actionable genes that I like to look at
and they're what's it called their sub
alleles. And when you find out what
they're deficient in, you start to
supplement with things like SAM-e,
S-adenosylmethionine,
methylated forms of vitamins,
L-methionine, the the proper balance of
B complex,
methylated forms of folic acid or folate
called methylfolate. And what happens is
now the body has the capacity to degrade
these neurotransmitters that are causing
this fight or flight. This group of
neurotransmitters called catecholamines
and the anxiousness that follows. And
you'll find that the majority of people
that suffer from idiopathic anxiety or
generalized anxiety because of low
serotonin, they also have gut issues.
You show me a person that's truly
depressed and I'll show you somebody
that's also suffering from severe gut
issues. Either gas or bloating or
diarrhea, constipation, irritability,
cramping because the same
neurotransmitters that affect these
emotional states also are responsible
for the motility of the gut, the speed
of the gut. This is the most overlooked
thing in all of bariatric medicine
because
people that believe that they have all
of these allergies. Well, I'm allergic
to wheat, soy, corn, dairy, blueberries,
bananas,
uh you know, gluten.
Yes, sometimes those individual
allergies do exist, but the majority of
time even if you talk to somebody who
says, "Yeah, I I I get bloated or I deal
with gas or cramping or diarrhea or
constipation or irritability. I deal
with all of these gut issues, irritable
bowel syndrome, uh Crohn's Crohn's
disease, ulcerative colitis." All these
names that we give to conditions of the
gut. When you ask them, "Well, what are
you allergic to?"
And they give you this laundry list of
things. And then you ask them another
question and say, "Well, if you're
really allergic to corn,
is there ever a time that you can eat
corn and not have a reaction?" Majority
of time people will say yes.
Okay, well, right there you know you
don't have an allergy. Allergies are not
transient, allergies are consistent.
Right? You don't wake up Monday morning
and being allergic to milk and then
you're unallergic on Wednesday afternoon
and then reallergic on Saturday morning.
But what happens when people have gut
issues that they can't explain is they
always correlate it to what they last
ate. And it's hard to make this
connection. They're like, "Well, wait a
second. I ate the same thing Monday and
I was fine and I ate the identical food
on Wednesday and I blew up like a tick."
So, this is not an allergy. This has to
do with the motility of the gut. So, if
you don't know what gene mutation you
have that is causing a deficiency, then
you don't know what to supplement with
to restore gut motility. But once you
do,
the gut goes back to its normal pace.
What's gut motility? It's the pace of
the gut. So, if you remember Henry Ford
was actually not made famous for the
automobile. He's made famous for
something called the assembly line. So,
the assembly line was just a glorified
conveyor belt, right? And when you
walked into his factory, they put a part
on it at one end and about every 6 ft
somebody stood and tinkered with that
part. So, it went to me, I tinkered with
it, it moved to the guy to my right, he
did something to it, moved to the guy to
his right, and by the time it reached
the end of that conveyor belt, it's
fully assembled. This is very analogous
to how the human intestinal tract works.
It's 30 ft long. It's a giant conveyor
belt. You put parts on it at one end as
they exit the stomach in a very acidic
environment and it moves slowly towards
the rectum and before it exits the
rectum, it's in a relatively alkaline
environment. So, instead of having
people standing along a conveyor belt,
you have bacteria that are graded by pH.
This sequence is very important.
So, imagine what would happen if Henry
Ford walked into his factory one day and
doubled the speed of the conveyor belt.
The entire assembly line would break
down. Not because there's anything wrong
with the parts, the contents, not
because there's anything wrong with the
people that are working there, the
bacteria, but because you changed the
speed. What if he went in there one day
and reversed the the conveyor belt? What
if he just ran it in the opposite
direction?
Screw up. Just It would screw the whole
thing up, right? So, by changing the
pace of the gut, the speed of the gut,
the conveyor belt, I've I've ruined this
sequence of events. And I spend a
lifetime trying to figure out what's
wrong with the parts, what's wrong with
the workers, what's wrong with the
conveyor belt itself. Nothing.
It's how quickly or slowly it's running
because the motility, this peristaltic
activity, is affected. And once you
supplement for this deficiency and you
return that activity to normal, you find
that
all of a sudden these strange allergies
eviscerate and all of this gas and
bloating and diarrhea and constipation
and irritability and all of this
inability to equate things that I'm
eating back to what is going on in my
gut seem to go away.
It's It's true with all kinds of
conditions. You know, we we have
subscribed in this world to the fact
that we are so affected by disease and
pathology. And once I get you to
to subscribe to the fact that you have a
disease and you can get you to subscribe
to a lifetime of medication.
You know, this is true in hypertension.
You know, it's another huge, you know,
we think genetically inherited disease.
And a lot of families have, you know,
grandfather had high blood pressure, um
dad had high blood pressure. Now the son
has high blood pressure. So, they go,
"Oh, it's genetic. It's genetically
inherited high blood pressure." Okay,
well,
what gene is being passed down from
these generations to cause this? Well,
they don't know.
Okay, well, then we know all of the
genes. So, if we don't know what gene it
is, then let's look at the methylation
genes. Let's look at the genes in the
human body that refine raw materials.
Because if you have a certain
deficiency, for example, in
hypertension, very often, not always,
but very often it's it's caused by
elevated levels of an amino acid called
homocysteine.
You have in your bloodstream right now,
I have in my bloodstream, every listener
to this podcast has homocysteine in
their blood. Because we we in in the
process of normally refining this amino
acid into something called methionine,
we
um we keep this level at a reasonable
level. But when you can't break
homocysteine down, it rises. When
homocysteine rises, it's very irritating
to what's called the endothelial lining
of the blood vessel. It in it irritates
the lining of the blood vessel. Well,
when you irritate a blood vessel, it
clamps down.
Well, if you make the pipes smaller in a
fixed system,
pressure goes up.
You have 63,000 mi of blood vessel in
your body. It doesn't take much
narrowing to drive pressure up. And so
these people end up with hypertension,
high blood pressure, and they go to the
doctor, and the doctor does an EKG, it's
normal. An EEG, it's normal. Stress EKG,
it's normal. Cardiac cath, normal. Heart
and lung sounds, normal. Dye contrast
study, normal. The entire cardiac
workup's normal.
And then they still start pounding on
the heart with medication because they
can't figure out why
the blood pressure's up, but they never
actually looked at what raw material was
missing in their body not allowing them
to bring homocysteine down and allowing
the vascular system to relax.
As the vascular system relaxes, pressure
returns to normal.
You spent 22 years
at that insurance company looking at the
database that you described. Um
and as you're as you're saying there,
you know,
much of the sort of medical profession
and I think most of society
Yeah, and I don't want to attack the
medical profession. I really you know,
I'm in no I am a huge lover and believer
in modern medicine. It's saved people
very close to me. I mean and trust me,
if I had a windshield at 20 miles an
hour, I want a surgeon, I want
painkillers, I'm going to the ER. But
there's been this kind of this it's not
a preventive approach to disease that
we've taken over the last couple of
decades. It really is, you know, to to
put a band-aid on something that's
that's emerged. And as you said at the
start of this conversation, these
predicaments, these um diseases emerge
decades before we even see the symptoms
often times. Um at the end of your 22
years at the insurance company, you
started to
look at these things which you call
modifiable risk factors.
Yes. What is a modifiable risk factor?
And what are the most common modifiable
risk factors in your view? Well, I mean,
one of the most common ones that I saw
was um modifiable risk factor is
it's a risk factor that you have
and if you changed it, it would have
modified it, it would have a
demonstrative impact on the trajectory
of your life. So, for example, anemia,
right? Low low hemoglobin, low red blood
cell count, low oxygen transport in the
blood will exacerbate just about any
condition that you have, right? So, if
you are hypertensive and anemic, if you
are diabetic and anemic, if you are
morbidly obese and anemic, um meaning
you have low blood oxygen because you
have low red blood cells, low
hemoglobin,
what if you could modify the anemia?
Well, if you could modify the anemia,
carry more oxygen in the blood, you'd be
much more resilient to all of these
conditions.
Right? So, the same thing is true with
dementia and Alzheimer's and and uh
cognitive function. As you impair
cognitive function, you increase the
incidence of all-cause mortality. So, a
modifiable risk factor would be
something like um looking at the levels
of vitamin D3 in the blood blood in the
body. So, it's estimated that roughly
50% of the world's population is
clinically deficient in vitamin D3. Why
is that important? Um well, vitamin D3
is the only vitamin that a human being
can make on our own. There's hundreds of
vitamins in your bloodstream right now.
You're only capable of making one.
And it's vitamin D3, cholecalciferol. We
make it from sunlight and cholesterol.
You don't even need to eat to make this
vitamin. There is not a single cell in
the entire human body that does not have
a receptor site for this vitamin. It
also acts like a hormone. It's calcium
transport molecule. It's enormously
impactful in your um immune system.
Clinical deficiency in vitamin D3 was at
one time the second leading cause of
morbidity in COVID. You know, when they
said COVID disproportionately affected
minorities. If you ever heard that, it's
true. So, how did COVID
disproportionately affect minorities? It
wasn't like the virus didn't start going
after certain minority populations.
Well, it actually did, but it wasn't
because they were not minorities. It had
to do with the pigment of their skin.
The darker the pigmentation of your
skin, the lower the vitamin D3. The
lower the vitamin D3, the more
compromised the immune system. The more
compromised the immune system, the more
susceptible you are to attack. That
suggests that if you have darker skin
like I do, that you should spend more
time in the sunlight. Yes, it does.
It absolutely does. I mean, you and I,
just based on our skin tone, if you and
I in a pair of board shorts went out and
spent 30 minutes in sunlight, I would
manufacture about 25,000 IUs,
international units of vitamin D3, you
would manufacture about 3,500. [ __ ]
hell, that's not fair.
It's not fair.
We can run faster.
But, you also
you also look better older and you don't
age, you don't get wrinkles as much, you
have better oily skin. There's some
trade-offs. So, so when you look at, you
know, African-American populations,
Latino populations, Middle Eastern
populations, they're the percentage of
vitamin D3 deficiency approaches 85%,
right? The truth is most of us are not
getting enough sun. It's not where that
we're getting too much. So, let's talk
about the depletion of this one
nutrient. Can I just ask them before we
move on to the depletion of that
nutrient?
Cuz I want to understand why that is.
I'm my guess was that because people
with darker skins have grown up in
sunlight, we spend more time in in the
sunlight, I'm guessing, which meant that
we adjusted our production of vitamin D3
to suit the environment we lived in.
Yeah, you actually have a better
barrier, right? You are um less
susceptible to skin damage from sunlight
than someone with lighter skin, right?
And so, if you actually look because I
used to be a population mortality
expert, um you know, the hot the longest
life expectancies um were centered right
around the equator of the earth. If you
look at most of the blue zones, they're
going to be
sort of closer to the equator of the
earth. They're going to be closer to
places where the sun shines longer
periods of time throughout the year.
The blue zones? The blue zones are
Sorry, the blue zones are areas of the
world where people live um
extraordinarily long life expectancies,
right? Mediterranean diets. So,
the longest life expectancies are
centered around the the equator. So, for
every 20° um uh
latitude, um cuz this is longitude,
every 20° latitude, there's a
precipitous drop in life expectancy
until you get to the poles,
where when I started in this industry, a
um the lowest the shortest life
expectancy on earth existed. So, when I
was born in 1970, a true Eskimo had a
56-year life expectancy. A 56-year life
expectancy had 56.
True Eskimo. So, these are these are at
the poles. Now, why? Because they would
go months without seeing the sun. And
when they did see the sun, they were
layered up. So, they had brittle bone
disease, they had autoimmune disease,
they had immunocompromised
conditions, all kinds of conditions that
go with severe depletion in vitamin D3.
And so, I would see this in the medical
record all the time, right? I would see
medical record after medical record, you
know, a patient has been had a decade or
longer of clinical deficiency in vitamin
D3. Well, when you deplete this nutrient
and you don't supplement for it. By the
way, vitamin D3 is so easy to supplement
for. Everybody should be taking vitamin
D3 unless you're getting adequate
sunlight.
5,000 IUs of D3 with 80 micrograms of
K2.
And you know, you you deplete this
nutrient, eventually you will develop
rheumatoid arthritis-like symptoms. Now,
you don't have rheumatoid arthritis, but
you have you have the same identical
symptoms when you're depleted in vitamin
D3. You start waking up sore and achy
like you had a workout the night before
when you haven't. The soles of your feet
and your ankles are tender when you get
out of bed in the morning to walk to the
bathroom, take your first pee. Um, your
your knees and hips and ankles start to
stiffen up. Then it goes to cross the
shoulders and eventually it's hard to
make a really tight fist. Well, if you
go to the wrong physician,
family medicine practitioner that's
seeing a lot of high volume of patients,
you start to give them that description,
they go, "You know what? You got you got
rheumatoid arthritis. I'm going to hit
you with something called
corticosteroids. I'm going to put you on
some prednisone first and then we're
going to transition you to a
corticosteroid like a methotrexate or
one of these
and and you're going to be fine. You
know, you you know, it's it's going to
push this off into the future." Well, we
knew that if you started corticosteroids
that at first they had an
anti-inflammatory effect, but you had
roughly 6 years and 1 day until you're
having a joint replacement. Because
first they're anti-inflammatory, but
then they eat the joint like a termite.
And so it was so accurate that if you
were a 60-year-old female and you were
misdiagnosed with rheumatoid arthritis
because you had a vitamin D3 deficiency,
I would artificially advance your age 6
years. I would schedule the joint
replacement that wasn't required, by the
way. I'll schedule the joint replacement
and then I would begin to reduce what's
called your ambulatory profile, how well
you ambulate, how well you move.
And we know now that sitting is the new
smoking, right? Sedentary lifestyle is
the leading cause of all cause
mortality. And so as I start to reduce
your ambulatory profile, I'm bringing
all of the diseases that exacerbate with
reduced motility.
So, if I back this up,
you were diagnosed with a condition that
you didn't have
because you had a deficiency in a very
simple nutrient. So, then you were put
on a medication that wasn't required.
This caused you to have surgery that you
didn't need because to replace a joint
that wasn't initially going to be
defective. This reduced your mobility
and it brought diseases forward that you
never would have caught and you died
early from a condition you never would
have had because you had a deficiency in
a nutrient that was misdiagnosed,
mistreated, and led to your early
demise. And I could give you hundreds of
examples like this, and this is why, if
you look at the 2016 Harvard study, the
2019 Johns Hopkins study,
medical error is the third leading cause
of death. Medical error?
Medical error. Is that misdiagnosis?
Misdiagnosis and medical error.
The average American
over 50, 52,
is on five prescription medications.
These are synthetic chemical
pharmaceuticals,
right? And in a lot of cases, we don't
know the long-term side effects of
these. In a lot of these cases, we
actually don't even know the mechanism
by which they work. If you actually open
the PDR that comes with the the the
disclaimer that comes with a lot of
these medications, you'll see that they
say mechanism of action unknown.
Well, it's a sleep medication. How does
it make me sleep? I don't know.
Just makes you sleep, right? In fact,
most people that are suffering from from
sleep issues are suffering from sleep
issues not because they can't sleep, not
because they're not tired, because their
mind is keeping them awake.
Right? If you have a gene mutation
called COMT,
catechol-O-methyltransferase,
then what happens to you is you lay down
to go to sleep,
and there's nothing more frustrating
than one spouse having this gene
mutation and one not, right?
god, I think you're talking about me and
my partner.
I'm the one that that I need some like
sound or something to go to sleep
because she's just out like a light.
There you go. See, and nothing's more
frustrating because so annoying. I
sometimes sleep in another room Okay, so
the reason why you're not falling asleep
is because when your environment quiets,
your mind wakes up.
And if you actually hone in on the kind
of things you're thinking about, you're
thinking about the most innocuous little
nonsense,
right? I mean, it's like did I get
everything on my grocery list? Did my
belt match my shoes today? Did I return
that email? It's nothing that couldn't
wait till the next day. 100%. Yeah, and
so and sometimes you can even catch
yourself going, "What am I doing?"
Thinking about the color of dishes I'm
going to have if I threw a party, which
I'm probably not going to throw. I just
like, how did I get down this rabbit
hole, right? And um this is because, you
know, the you're not quieting the mind
at the pace that you are
exciting the mind. So, in other words,
when you lay down to go to sleep and
your environment quiets, your mind
starts to wake up. So, you need to be
distracted so that your mind doesn't
continue to run. But, if you just put
the right amino acid balance, in fact, I
would bet my career you have this gene
mutation.
I will pay for your test if you don't.
It's $599. It's a cheek swab you do once
in your lifetime and it will tell you if
you have this gene mutation, COMT. And
if you do, I'll tell you exactly what
supplement to take and it will become a
permanent thing of your past.
What supplement should I take?
Don't end your sentence there, Gary.
So, it's called L-methionine.
Oh, I've heard And you take
L-methionine, you take methylfolate,
and depending on where the gene break is
and how severe it is, you add you may
add something called SAM-e,
S-adenosylmethionine.
And these sound like fancy names,
they're just fancy names for vitamins
and amino acids. They you all of these
are in your bloodstream right now. So,
when you look at the sequence of breaks
that somebody has, then you can tell
them exactly what supplement to take.
When they take the supplement, their
body's no longer deficient.
Right? Deficiencies over time express
themselves as all kinds of things. You
know, there's a lot of people that can't
reach elevated emotional states for any
prolonged period of time. This is
because mood and emotional states are
recipes, just like a
you know, a chef
bakes a recipe. But, if you went to a
bakery chef and you said,
"You can bake whatever you want.
You just can't use butter."
Okay, doesn't sound like a big deal.
It's just one ingredient. But, think of
the number of cookies, pastries, pies,
brownies, you know, that it would
affect. It would affect so many
different recipes just by removing one
ingredient. This is the same thing that
happens in human beings. If you couldn't
use serotonin to assemble mood, okay,
now any emotional state that requires
that neurotransmitter as a part of its
structure, you can't assemble.
And as it relates to that mutation, you
when when you people hear the term
mutation, they think of it as being
something that's happened in me. And I'm
maybe, you know,
one of a few that have that mutation.
Mutation sounds like a uh Yeah, it does
sound it sounds it does sound like an
alien's about to start like growing out
of your stomach.
it sounds like it you know, my sister
won't have it and it's just me.
Okay, so a gene mutation means that, you
know, we we get a copy of our genes from
each parent. Yeah. Right? And then these
the the copy of these genes is passed
down to us. And we know you know, most
of us are familiar with basic genetics.
Eye color, skin color, detached ear
lobes. Um but there's nothing you can do
with that information.
So beyond your ancestry, you know,
whether you got Irish heritage or Native
American Indian or or what have you. I
mean, those are if you did a 23andMe,
you'd be able to find your ancestry,
which is also your genetic history.
That's not actionable information.
When you look at the genes of
methylation,
right? And there are several of them. I
look at five majors and a few minors.
When you look at the genes of
methylation, these are the genes that
code for how materials are taken into
the body, are refined into the usable
form.
And these are not mutations that you're
going to suffer from. What they do is
they they they
cause deficiencies to arise in the body.
And it's this deficiency that leads to
the expression of these conditions.
And so when you can't adequately
methylate neurotransmitters, you have a
deficiency in a certain
neurotransmitter. Any mood, any
emotional state that requires that
neurotransmitter, you can't assemble. If
you have a deficiency in the ability to
quiet the mind, then you have excess um
neurotransmitters in the brain, which
cause it to stay in awaken state. So,
that gene that is responsible for my
loud mind when I go to sleep.
Mhm.
Do you have any idea the amount of
people that have that particular gene?
Well, 44% of the world's population has
a gene mutation called MTHFR,
methylene tetrahydrofolate reductase.
This is a
genetic mutation that impairs the
ability to convert folate into
methylfolate or folic acid into
methylfolate.
And that might not sound like a big
deal, but folic acid is one of the most
prevalent nutrients in the human diet.
And the thing about folic acid is that
folic acid is an entirely man-made
chemical.
Folic acid is not found anywhere on the
surface of the earth. You can't find
folic acid anywhere naturally in nature.
And yet, we give folic acid
to pregnant women when they get pregnant
because we tell pregnant women that
folic acid prevents neural tube defects.
Well, that's patently false. Folic acid
doesn't prevent anything. Folic acid has
to be converted
first into tetrahydrofolate then
dihydrofolate, but eventually it becomes
something called methylfolate. And that
prevents a neural tube defect. Well,
what if like 44% of the population and
44% of women, this woman has this gene
mutation and you give her folic acid,
the man-made version of folate, and she
can't convert it into methylfolate. This
is where postpartum depression develops.
And you know, I have not seen a single
peer-reviewed published clinical study
linking elevated levels of of
uh
hormones in female pregnancy to
postpartum depression. But if you give a
woman that can't methylate folic acid
1,400% of the daily allowance of folic
acid and she can't break it down, then
she goes nuts. And then eventually the
pregnancy ends, the depression goes
away, and so So blames it on the
pregnancy, not on the vitamin.
And you know, we do this over and over
and over again. You know, we have in in
in the modern industrial world, we try
to synthesize what occurs naturally in
nature in a laboratory. You know,
there's three types of B12, right?
Adenosylcobalamin, Hydroxocobalamin,
Methylcobalamin. These forms of B12
occur naturally in nature. There's one
that we make synthetically in a
laboratory. It's called Cyanocobalamin.
We make it from hydrogen cyanide.
It is useless in the human body. The
human body actually has to take it and
convert it into the active form of B12
called Hydroxocobalamin. And so, a lot
of times the supplements that we're
taking us are causing more harm than
good and we're taking them because the
doctor said, "Well, I'm pregnant. My
OBGYN told me to take this synthetic
chemical called folic acid which it's
always beyond me why anyone would think
that something that we make in a
laboratory that's entirely synthetic
that isn't natural, that isn't found
anywhere on the surface of the earth
could ever be required for optimal
health."
I mean, just in its on its surface that
sounds
strange to me. But,
you know, yet we do and we don't
understand this process of methylation.
So if you Once you understand where your
genetic mutations are, where the genetic
inability to refine raw materials is,
you can go about supplementing targeted
supplementing for that deficiency. So
you would recommend people take a
genetic test to find out these answers,
right?
everyone take that test once in their
lifetime. You know, I
I'm I'm in the camp that we're as humans
we're not broken. Like we're not broken.
You know what I mean? And so whenever
there's something going on in my body or
you know, a way that I am or a habit I
have that I'm like, "Why do I do that?"
I'm always trying to figure out the sort
of I guess the ancestral reason why that
might have helped me to survive or
what's going on. So when I hear
mutation, it's it sounds a little bit
like broken to Yeah, yeah. So I
shouldn't use the I mean, we we use the
term mutation, but basically, you know,
in our ancestry, right? We pass on our
entire genetic code. Which a lot of that
is hair color, eye color, skin color,
you know, our our our heritage. But we
also pass on how our body refines
certain raw materials. And it's not to
say that it's good or or or bad or or
broken or fixed, but there are certain
families and human beings that have an
inability to refine certain raw
materials. And if we could be aware of
this, it is astounding what happens to
human beings when you just give their
body the raw material to do its job. You
know, lots of people that have attention
deficit disorder or have trouble
sleeping will
also have a trouble trouble with
prioritization. They just don't know it.
They'll say things like, "I work really
well under pressure." Right, most
entrepreneurs say, "I work really well
under pressure." Do you say that? Oh my
god. Okay. So let me I only work when
there is pressure.
So I was like getting to school that
we'd only do the test when you know,
there was an hour left to go or you
know, the homework or whatever. Yeah, so
many entrepreneurs are that way. And and
when you say you work really well under
pressure, physiologically what you're
saying is, "I lack the ability to set
priorities internally. So I use external
pressure to set my priorities." And why
is that? It's because when you don't
have the right methylated nutrients in
the body, you lend equal weight to every
thought that comes into your mind.
Right? So you could be working on
you know, the deal, the joint venture,
business closing of a lifetime. Right?
And you got the contract and you have 45
minutes to get it back to your lawyer
you know, the deal's permanently going
to go away. This is a life-changing
deal. You've
waited for this your entire life. It's a
very meaningful event. You're working
your way through this legal document and
you look over at your phone and there's
an Instagram message. And you're like,
"Oh, that's my neighbor's cousin's kid
fishing in the lake.
You know, I wonder if he catches a
fish."
So you start looking at it and you're
like to he's still casting. Oh, he
didn't catch it that time. Now,
meanwhile,
this has gone from 45 minutes to 35
minutes.
And now it's down to 25 minutes. And all
of a sudden you go,
"Oh, no crap." You turn the phone off,
which didn't mean anything anyway, and
you focus all of your attention and
because you're very intelligent and you
and you execute and you can hyperfocus,
you hyperfocus on this and you worm your
way through it. And 1 minute before the
deadline, you hit the send button.
Lawyer gets it. The deal goes through
and you go,
"I work really well under pressure."
What what's that called? That process
you described there is many people
describe that as procrastination. Mhm.
It's procrastination, but it's
procrastination because you give equal
weight to all of these different
variants that come into your and that
come into your your field. So, you
actually give equal priority
to very disequal events. But also, you
know, sometimes if I'm looking at that
contract, the contract clause is a
little bit difficult. And my attempt to
maybe dis escape discomfort would be
I'll just go do the dishes. Mhm. Right?
And that And so, I had Nir Eyal on the
podcast. He wrote a book called
Indistractable and he says we're
creatures that we're not we're not
pleasure-seeking creatures. We're
creatures that are avoiding discomfort
essentially. I think that aging
is the aggressive pursuit of comfort.
Could not agree with you more.
Let's use Dana White as an example.
Okay. Because, you know, the reason why
I came across your work is because of a
clip that
you know, involved Dana White and I'm
sure you I know you get this a lot
because I've seen you um be asked about
this in interviews, but for context for
anybody listening, I don't know where I
was or Ah, now I know what happened. My
friend sent into a WhatsApp group a clip
of Dana White talking about you. Mhm.
And that's the clip that made me
go down the rabbit hole. Oh. I watched
that clip. I then did some research. I
then watched a series of videos of you
online talking about health and I
watched you asking audience members to
stand up and name the you know the
health issue they were suffering and you
on the spot told them what was missing
from that their life, their diet,
whatever it might have been. You kind of
diagnosed them in a way of Um and then I
reached out to you on Instagram and
that's why you're here. But if we go
back to the start of that, it was that
story that Dana White told that had me
so compelled to to reach out to you. For
anybody that doesn't know and there will
be some people that don't know, Dana
White is the president of the UFC which
is the the
the the big fighting tournament where
everybody kicks each other's heads in.
So
what's your take on the the Dana White
story? So, Dana White is a an example, I
mean he's just a celebrity example, but
he is a shining example of the vast
number of people, you know, men and
women in his age category
that have given up on the capacity to
thrive. They've accepted that they have
hypothyroidism, hypertension, they wake
up sore and aching in the mornings, that
they don't have a response to exercise,
they have a little bit of spare tire,
they're brain foggy, they're on three or
four medications. In his case he was on
seven
medications at the time, three of which
were for blood pressure.
Um he was on, you know, I think a
thyroid medication, was also on He's
been very public about this by the way.
And and again I have to say I'm not
licensed to practice medicine, so it was
my clinical team that that came up with
the diagnosis and I communicated it to
Dana. Um I do train physicians to read
blood work and genetic testing, but I
can't practice medicine.
But the the point is that
when I met Dana
all he wanted to do was for me to
predict his life expectancy. And I
hadn't done that in almost seven years.
I left that industry for a reason, I
don't do it anymore. The test that I do
does not predict life expectancy. The
genetic test and the blood work that I
do will not tell you how long you're
going to live. I have no interest in
predicting death anymore. I only have an
interest in extending life.
And
you know, when when Dana was only
interested in me predicting his death.
So, I said, "Okay, for Dana White, I'll
come out. I'll meet with you.
I'll do a blood test on you, a gene test
on you. I'll pull all your medical
records, and I'll give you your life
expectancy."
But, what I did was went out and got his
blood work and his gene test, and
um I was actually in bed
at 1:30 in the morning when the lab was
running his blood work. And I've had
seven life-threatening alert calls um in
the middle of the night because when you
drop blood work off at the lab, the lab
runs it through the night. If they find
a life-threatening alert, they call the
account holder, right? So, um I own the
company. I was on the account. So,
LabCorp calls us at 1:00, 1:30 in the
morning, says, "Hey, we have a
life-threatening alert on a patient." I
was like, "Whoa.
Um
what's this patient's name?" They said,
"Last name's White." I said,
"Dana White?" They said, "Yeah." And I
go, "Whoa. What's the uh
life-threatening alert?" They said,
"Triglycerides are almost 800."
Now, triglycerides are a measure of
blood fat. Okay? It shouldn't be above
149.
At 200 or 300, this is a
cataclysmic level in the blood,
especially in a fasted state. Okay, we
pulled his blood in a fasted state. They
weren't 400. They weren't 500. They
weren't 600. They weren't 700. They were
like 768.
So, they were I mean, this is an
enormous number. And so, I said,
"Okay, uh I need to get the blood work
over to the, you know, to the doctor."
And when they sent the um the blood work
into the portal,
I then saw that he was insulin
resistant. He was hyperinsulinemic. He
was prediabetic. He had skyrocketing
levels of cholesterol. He had He was
hypertriglyceridemic. He was hyper um
homocystinemic. This homocysteine that I
told you elevates and causes the blood
vessels to constrict. Um I mean, he had
all of these conditions. I literally at
that moment booked a flight
for 7:30 or 8:30 in the morning
to head out and see him.
And
because I said I need to go see him in
person. And I remember I think his
assistant called me and I was at the
airport and she said, "Hey, Dana wants
to know if his life expectancy is in." I
go, "Well,
I'm on my way to see him, you know. Um
And she goes, "Oh god, is it like that?"
I said, "Yeah, it's like that."
And uh so I flew out to see him and I
sat down with Dana.
And
when we talked about the blood work, I
didn't even explain the levels. I
explained the symptom.
Um I did not know that he was on a CPAP
machine, but I said, "I am surprised
that you can actually sleep through the
night because he was so hypoxic.
Um red blood cell count, hemoglobin
levels.
Uh I'm surprised you could even sleep
through the night without like just
waking up choking, gagging." He's like,
"Dude, I'm on a CPAP machine. I wake up
every night. I throw up in the middle of
the night. I throw up so much I'm losing
my voice."
Um And I said, "This level of
coagulation triglycerides in the
bloodstream will surprise you can't even
bend down and tie your shoes. That's not
painful to tie your shoes. Not that it's
not restrictive to tie your shoes. It's
not painful. Like it doesn't feel like
the skin's going to peel off your legs."
And he went, "What the
I mean, he
slammed his hand down. He was like, "How
did you You know, how did you know
that?" And I said, "Dana, your level of
brain fog and fatigue right now has got
to be at a crushing level of fatigue. I
don't know how The only thing getting
you through the day is your own stubborn
willpower. And I'm surprised you can
remember anything from one minute to the
next." And his whole staff was like,
"Dude, he's so forgetful. He passes out
in meetings. He's sleeping on the
planes. He's gagging, snoring."
Um these were not things I necessarily
knew about him. So, I began to describe
all the
outcomes of these kinds of conditions.
And I said, "Look,
um
if if you don't do what we're going to
ask you to do for the next 10 weeks,
you know, based on this blood work and
the medical records that we pulled for
the previous 10 years and the
demographic data we pulled for 10 years,
you have a life expectancy of 10.4
years.
Um, you know, for a 52-year-old man to
realize he's not going to make it out of
his 60s,
a big realization. And he flipped a
switch, a level of discipline that, you
know, I haven't seen in a patient a long
time. He goes, "Dude, I'll do whatever
you tell me to do."
So, we wrote a prescription ketogenic
diet. I I I'm a fan of the keto diet. I
don't think everybody needs to be on the
keto diet, but
um, my prescription ketogenic diet, we
wrote a keto diet right down to the
grocery list, keto reset diet. And I
said, "If it's literally if it's not on
here, you can't eat it, Dana. This is
your grocery list. You go to the store,
you buy this. You send your chef to the
store to buy this. You make this. If
it's not this recipe, if it's not on
here, you literally can't eat it. Your
only leeway is water
and the supplements."
And um,
and we started uh a process of of
balancing hormones, controlling his
glycemic index, of using amino acids to
bring down his level of homocysteine, to
actually try to fix the insulin
resistance, to reduce his triglycerides.
And in 10 weeks,
he had a such a material change in his
blood work. I forget how much weight he
lost. I think he had lost almost 28 or
30 lbs at that time. He's over 40 lbs
now.
Um, by the end of the fifth month, he
was completely off of every prescription
medication he was on. He's down 44 lbs.
He lost the you know, he's no longer
using the CPAP machine. He no longer is
pre-diabetic. He no longer has insulin
resistance. He no longer has
life-threatening levels of triglyceride.
In fact, they're normal. His kidney
function improved. His liver function
improved. His immune system
strengthened. He feels like a
35-year-old man again. His skin tone all
improved. Um, his blood pressure
returned to normal. He's not on any
blood pressure medication.
Uh, so his blood pressure returned to
normal and he was like,
"Dude, I had no idea I could feel this
good. I feel freaking amazing." And his
life expectancy?
Almost tripled.
Almost tripled?
Almost tripled. Just under 30 years.
When I heard the story about Dana White
and I saw he'd gone from respectfully
being a man that had a little bit of
weight to to having this these six-pack
abs on Instagram. Of course, the
six-pack isn't the the outcome. It's as
you've said, it's the stuff going on
inside him. That's really the
transformation.
It it left me with the question like,
okay, I I heard the keto bit. But what
can someone who's just heard that at
home, where do they start with getting
extending their life by triple and
getting the
So, you know, he also started something
called the superhuman protocol.
And superhuman protocol is using
magnetism, oxygen, and light, right? So,
the only things that we really get from
Mother Nature, the the the big benefit
we get from Mother Nature is we get
magnetism from the Earth, we get oxygen
from the air, we get light from the sun.
The truth is, most of us are not
contacting the surface of the Earth that
much anymore. So, he bought $150,000
worth of equipment, a PMF mat, an oxygen
what's called a hypermax oxygen to do
exercise with oxygen therapy, and a red
light therapy bed. And I had him use
that equipment every single day, 7 days
a week.
But if your listeners want to do it for
free,
you can take off your shoes and contact
the surface of the Earth. And I'm
talking about bare feet on soil, dirt,
grass, sand. Because earthing and
grounding is a very real thing. We
actually discharge into the Earth. We
actually human beings built up a charge.
Do you know that pH, the acid alkaline
scale, pH stands for potential hydrogen.
It's a charge. It's a complete fallacy
that you can get alkaline by drinking
alkaline water. That's the biggest
marketing myth ever sold to the public.
Um
but you can get alkaline by contacting
the surface of the Earth. So, if you
don't have 150 grand, which I don't
expect anybody listening to this podcast
to spend 150 grand, but he did. I said,
you need a magnet you need a PMF mat so
that you can be alkaline. You need to
spend 10 minutes a day breathing um 95%
O2 under mild exercise and you need to
lay in a red light therapy bed. So,
in the absence of the superhuman
protocol, you can become superhuman by
contacting the Earth and by learning to
do breath work.
Let's talk about breath work. I spend 8
minutes every day doing a very specific
series of breath work and I'll teach it
to you now. You're You said your wife is
certified in? Yeah, my partner she's a
she's a breath What practitioner? Um
I've done breath work with her. I've
done breath work with a few people but
no one's ever had the profound impact on
me through breath work that she has.
I've never shouted her out before so I
probably should. Her Instagram is
@meloai
for anybody that's interested in breath
work. People do not realize the power of
something that is so accessible, so
free, and so easy to do, right? They
They want things to be more complicated
but it's not. And when I said the
presence of oxygen is the absence of
disease, it's absolutely true. Remember
that every elevated emotional state that
a human being can experience actually
has in its molecular structure
oxygen is a component of that emotion.
So, if you look at the difference
between passion, elation, joy, arousal,
libido
and anger for example, it's usually only
one neurotransmitter and the presence of
oxygen. The reason why no human being
has ever woken up laughing is because
you don't have the oxidative state to
experience laughter right out of deep
sleep. But can you wake up angry?
Yes. Because anger doesn't require
oxygen. So, every morning contact the
surface of the Earth and then spend 8
minutes doing I do a Wim Hof style
breath work. I give credit where
credit's due. He's the father of breath
work as far as I'm concerned. So, I do
three rounds of 30 deep breaths.
Like obnoxiously deep breaths.
And I start by trying to take my belly
button and pull my belly button out
towards the wall. Imagine there's a
string pulling your belly button towards
the wall
and then you
you fill from the lobes of the lung to
the apex of the lung and then you exhale
and just relax.
God knows what they think we're doing
out there.
Right outside this podcast. They're
like, "A bunch of freaks. I knew it was
a cult." Um
I knew I knew he was a cult leader. But
um so you do three rounds of 30 breaths.
On the 30th breath you exhale and you
hold. Allow the carbohydrate receptor to
reset. When you don't feel you can hold
anymore, you take a deep breath in.
You hold again and then you let it out
slow.
And you start again. I would suggest
that you start with three rounds of five
breaths. Then work to 10, 15, 20, 25,
and 30. If you get light-headed, this is
a good sign that the oxygen tension is
changing in your brain. If your fingers
and toes get tingly, this is a good sign
that you're changing the oxygen tension.
If you feel some kind of heat
temperature change in your neck, these
are all great signs. You will get to the
point where you can actually hold your
breath for two or three minutes,
sometimes four minutes between rounds of
breath work. Um and then the last thing
is to expose yourself to natural
sunlight. First thing in the morning,
the first 45 minutes of the day God
gives us a very, very special type of
light. It's called first light. There's
no UVA, there's no UVB rays in this
light. Um so that it's not the damaging
rays from the sun. It still generates
vitamin D3. It has a positive effect on
cortisol, on vitamin D3. First light is
the best way to reset your circadian
rhythm. So by contacting the surface of
the earth, doing breath work, and
getting first light, you can get to the
same place that Dana White did with 150
grand in equipment. What about oxygen
masks? Cuz I I'll be honest, when I read
when I read um about the Dana story, I
went on Amazon soon after and I was
like, "I'm just going to buy an oxygen
canister." Good idea, bad idea? Um so
what you want to do is um you know, you
get an oxygen concentrator, which takes
21% oxygen from, which is what the
concentration at sea level. It turns it
into 95% O2 and it fills this bag. And
it can refill this bag over and over and
over again. Okay, I use one called a
HyperMax. You can see it on my
Instagram.
And, um, you turn you plug it in, you
turn it on, it fills this bag, and then
you go and you put an oxygen mask on,
and you exercise for 10 minutes. Only 10
minutes. Cycle for 3 minutes, s- uh,
sprint for 30 seconds, cycle for 3
minutes, sprint for 30 seconds, cycle 3
minutes, sprint 30 seconds, and you're
done. And what this does is it raises
something called the partial pressure of
the the storage of oxygen in your blood.
The only two-time two-time Nobel
laureate prize winner in in medicine,
Dr. Otto Warburg, won both of his Nobel
prizes for his work in exercise with
oxygen therapy. You want to be a
superhuman? Do mild exercise every day
while breathing 95% O2. And it's
important that you're exercising.
And then, after that, you move into a
red light therapy bed,
photobiomodulation.
Um, so, you know, if you don't have
access to a HyperMax oxygen machine,
just do the breath work. Get the breath
in, you know, exchange the oxygen
tension in the tissues, and expose
yourself to first light.
What about cold cold water plunging? So,
I'm a huge fan of cold water plunging,
but probably not for the reasons why you
think. You know, um, I also sit on the
board of the NFL, um,
uh, alumni association athletica as a
health services director. You know,
there there was a time when we used to
think that putting athletes in cold
water after exercise was good because of
its anti-inflammatory effects. We know
now that that's only about 15% of the
benefit. The majority of the benefit
comes from something called a cold shock
protein. If you really want to be
fascinated, Google cold shock proteins.
These are reserved proteins that are in
your liver. They're dumped into the
bloodstream in effort to save your life
when you put yourself in cold water.
They scour the body of free radical
oxidation. They increase the rate of
protein synthesis, muscle repair. They
are free. You get them when you put
yourself in cold water. Um, I don't know
what the Celsius conversion is, but I
use 50° for 3 minutes.
Minimum 6 minutes maximum. Cold? Yes.
It's It's actually not that cold. I
mean, you know, I see people getting in
37, 38° water. There's no evidence that
I've read that shows that colder is
better. You get a peripheral
vasoconstriction, so it forces all the
oxygen into the core and up to the
brain. Um, and you ask you get an
activation of something called brown
fat, right? Um, thermogenesis comes from
brown fat. And for the women that are
listening, for some reason I seem to
insnare the women when I say this.
Remember that the definition of a
calorie is a measure of heat. Right? I
mean, the definition of a calorie is the
amount of energy it takes to raise 1
cubic centimeter of water 1° centigrade.
So, if if if a calorie is a measure of
heat, then this means that when heat's
leaving your body, calories are leaving
your body. So, if there is nothing
nothing, no amount of exercise, hits
cardio, no type of cardiovascular or
weight training that comes anywhere
close to immersing yourself in cold
water in terms of what will strip fat
off your body fast. If you want to strip
fat off your body,
get in cold water 3 to 6 minutes a day.
That's fascinating. Because because the
oxygen rushes to my head, that's why it
has a really profound impact on mood.
That's why it has a very profound impact
on mood. Because if you think about it,
what's the reason why we need deep
sleep? What happens in deep sleep that's
so special? There's a secondary oxygen
transfer. We transfer oxygen from the
periphery, from the extremities, to the
brain. Remember, the brain's a
non-metabolic organ.
So, in other words, it's unlike a
muscle. If I pick up a weight and start
to work out my muscle, my arm, my body
will send more blood, more amino acids,
more oxygen to that muscle because it's
working. Well, if I'm sitting at my
computer and I'm watching a reruns of
The Simpsons,
or I'm sitting at my computer and I'm
solving the most complex joint venture
agreement, partnership agreement with
all kinds of mathematical equations, my
brain gets the same amount of nutrients.
Same amount of blood flow, same amount
of oxygen. So, it eats the same meal
whether or not it's in a dead sprint or
whether or not it's just chilling on the
couch. Except in deep sleep and when
you're in cold water because it's
forcing the oxygen up to the brain.
You said earlier about
about comfort. Yes. I I was speaking to
someone yesterday about this thing
called we he referred to it as the
comfort crisis and how
you know, as we've become more
civ- I'd say civilized but I don't know
if that's the right terminology. As
we've become more advanced
technologically as humans, we can make
our lives increasingly more comfortable.
Correct. Sounds like a good thing.
Terrible. It accelerates aging in every
form. I mean, aging is the aggressive
pursuit of comfort. We have got to stop
telling grandma not to go outside it's
too hot, not to go outside it's too
cold, just to lay down, just to relax,
to eat at the very first pang of hunger.
This is collapsing all of our own
natural defense mechanisms. You know, if
we don't load our bones, they don't
strengthen. If you don't tear a muscle,
it doesn't grow. If you don't challenge
the immune system, it weakens.
And so, stress is very often very good
for the body.
Thermal stress, um you know,
weight-bearing exercise, breathwork,
these things put stressors into the body
that are very they have a very positive
effect at strengthening you. We want to
regulate everything now. We regulate our
temperature. We go from a you know,
temperature-controlled office to a
temperature-controlled car to a
temperature-controlled home.
You know, we don't we don't
thermoregulate anymore. I mean, you
know, usually when you when I ask people
to start taking cold showers, they take
their first cold shower, they never do
it again. Why? Cuz they don't want to be
uncomfortable.
And so, when you learn to deal
and become comfortable with being
uncomfortable,
this is like a metaphor for life. It's
almost like yoga. If you've ever done
really intense yoga and you're holding a
yoga pose and you're you're trying to
remain calm and focus on your breath
while your body's in intense pain. Now,
you're not in any risk, but your ass
feels like it's going to peel off your
legs and your hamstrings are firing and
you're sweating and you're shaking and
you're doing this thing that's called
the candlestick, but it's really
painful. And if you can mean maintain
calm and and and breathe through a
situation like that, what happens 4
hours later when you get a nasty
Instagram message? Nothing.
Doesn't shift your mood. And if we don't
learn to control our emotional state, we
will never control our future.
You know, MIT did an incredible clinical
study that showed that the amygdala of
the brain, which is where we experience
emotion,
is the sole gateway to an area of the
brain called the hippocampus, which is
where it we hold our memories.
So, just imagine that the emotional
center of the brain is the sole gateway
to the memory of the brain.
This is why if you've ever had an
argument with your spouse, you can
always recall with incredible accuracy
every other time they've made you feel
this way. You know, you did this on
September 21st. You did this when we
were on the boat with my boys. You did
this at
um you know, our Christmas holiday party
four Christmases ago cuz because that
emotion is linked to that memory. So,
you can recall that memory very
accurately. Well, our memory, our
hippocampus, is what projects into the
prefrontal cortex. It determines our
future. It's our conscience.
So, this means if emotion is the only
gateway to memory and memory projects to
our conscience, which is our which is
our future,
this means that your current emotional
state
determines your future.
That's a biophysiologic fact.
So, like for example, if you had an
argument with your spouse on the way to
work and you get out of the car and you
slam the door and you walk into the
office, when you break the plane of the
door of that office, the only memories
you can recall about the office at that
moment are negative.
You're going to walk through the door of
the office, you'll be like, they don't
respect me around here. I'm going to
have a stern talking to management
today. You know, my office better not
you know, you know, nobody better be at
my desk and you know what, Mary better
not run into me today cuz she doesn't
respect me. You can just start going
through all the negative things about
the office. The The didn't do anything
to you. How do I prevent that?
your
You learn to control your emotion. How?
Well, first you start by putting the
right nutrients into the body that
allows you to achieve elevated emotional
states.
And you learn to do things like when you
feel like you are beginning to lose
control of your emotional state, you you
you actually break that cycle. I usually
do it with breathwork. Mhm. Um and so
um you know, first it begins by having
the right raw materials, but this is
just taking you back to the cold plunge.
If you can start your day in an elevated
emotional state, if anybody listening to
this has ever really done a cold plunge,
tell me if you were ever in a bad mood
getting out of a cold plunge. Just try
to be in a bad mood getting out of a
cold plunge. They say if you want to
cure depression, push somebody in cold
water. You know, um
and it's so true. You're in such an
elevated emotional state. You're like,
"Wow." Now you go cruising into the day
and get a little negative, you know,
Instagram message and your you know,
spouse calls you and tells you she
forgot what you wanted to get at the
grocery store and you get to work and
you got a little problem at the office.
These things roll off your back instead
of shifting your state, which now shifts
your memory, which now changes the
trajectory of your prefrontal cortex,
which affects your future.
I do a lot of traveling, Gary.
I travel all over the world all the
time. Oh, it's one of my favorites.
Yeah, you travel a lot? Tons. You've got
a bit of a system for traveling because
when I travel, I feel like [ __ ] Oh, I
feel amazing when I travel.
What do
And I post all about it on my Instagram.
You know, all I do is teach on
Instagram, but you know, I went Miami,
Atlanta, New York, London, Stadt,
Switzerland, Dubai, Dubai, Miami, Miami,
Vegas. I would I got I I I got up at
4:00 this morning to come here. I mean,
I I landed here at I think 7:15 this
morning. And you're flying out of here?
I'm flying out of here now. In 5
minutes? I'm flying out of here in 5
minutes and I'm going on a red-eye back
to Miami.
And you feel good when you travel and I
feel like [ __ ] What do you think we're
doing differently if you were to guess?
Okay, so there's three things that I
that you can do when you travel. First
and foremost, and I don't know why
anybody talks about this, is that you
know everybody talks about waking with
the sun which I'm a big believer in
or forcing yourself to stay up to try to
get onto a new time zone. When you
change time zones, the single most
important thing that you can do
is preserve your sleeping window. Do not
eat during your normal sleeping window.
Let me tell you what I mean. Let's say
that you're on the East Coast, you live
in New York
and you go to bed at 10:00 and you get
up at 6:00 a.m.
Okay, you go to bed at 10:00 p.m. Get up
at 6:00 a.m. Most people go to bed at
midnight get up at 6:00 a.m. So let's
say you go to bed 10:00 you get up 6:00
a.m. And now you go to London.
Okay, so now London is depending on the
time of the year 6 hours ahead.
If you eat
during 10:00 p.m. to 6:00 a.m. New York
time
there is zero chance you will adjust to
that time zone. We are more tied to our
digestion in terms of our circadian
rhythm than we are to the sleep-wake
cycle of the sun. So in other words, if
I fly to London and I start eating
when it's 3:30 in the morning my time
my body goes what the heck are you
doing? We're having steak and eggs and a
champagne? It's 3:30 in the morning.
Right? Your circadian rhythm is screwed
up. So shift your sleeping window and
preserve that sleeping window in your
new time zone and do not eat during
those times. So in other words, in
London that would be
6:00 a.m. to noon. So between 6:00 a.m.
and noon I'm not going to eat. I'll have
coffee or I'll have water
or fluids, but I will not start to eat
until noon. And how long do I preserve
that window?
Well,
depending on how long you're going to be
there. Usually I'm only if you're there
a week or less, preserve your sleeping
window the entire week that you're
there. When you're there for more than 7
to 10 days, then you need to really
adjust to that time zone.
What happens physiologically if I don't?
If you don't, you will you will
irrevocably mess up your circadian
rhythm. I I just sleep just just just
imagine it. So let's say you lived in
New York and you didn't travel. You go
to bed at 10:00 and you wake up at 6:00
a.m. Try for three nights setting an
alarm for 3:30 in the morning. Get up,
eat a big breakfast at 3:30, and try to
go back to bed.
And watch what happens to your sleep
cycle, right? You'll destroy it. So, we
don't we preserve our sleeping window.
The other thing is I fast on domestic
flights.
I don't care what time or where I'm
going. If I fly anywhere in the
continental United States, I fast on
airplanes. So, I I allow myself um you
know, water. I I hydrate and I have
black coffee. On international flights,
I just came back from Dubai. It was 16
hours. I ate on that plane.
Um and then for flights that are more
than an hour, every hour on the hour, I
get up out of my seat. I don't care how
weird it looks. I go to the back of the
plane. I do 25 air squats. I go either
into the bathroom or in the back of the
plane. I do 25 deep breaths.
On a 10-hour flight, I'll do 250 deep
breaths and 250 air squats over the
course of a 10-hour um flight. Feel
amazing.
And then I eat fats and proteins on
flights.
Carbohydrates at altitude are terrible
for you, and that's usually where all
the salt hides. Remember that you know,
there's there are essential fatty acids,
meaning they're essential for life.
There's two of them. Um if you don't get
these fatty acids, you'll die. There's
nine essential amino acids. They're
proteins. They're essential for life. If
you don't get these nine
essential amino acids, you'll die. There
is no such thing as an essential
carbohydrate.
Why Why are carbs so bad at in the air?
Um carbs are bad in the air because as
soon as you divert blood from your brain
to digestion. Let's not forget, it's a
30-ft long tube. The higher the the the
consumption of carbohydrate, the more
blood floods to your gut.
going to feel like crap.
So, now you're seated and your gut is
flooded with blood. It's all come from
your brain. So, now you're tired, you're
not focused, you're exhausted, and
you're seated. So, you're it this isn't
a good place to be tired cuz you're not
going to get good sleep.
Right? So, you So, I put I set a huge
priority on energy. Energy is a huge
priority to me. So, when I look at food,
I look at it two ways. It's going to
serve me or it's going to steal from me.
When I'm I'm flying first class back to
Miami tonight. It's a red eye. I'm going
to actually use that time to sleep. I'm
not going to waste it on eating because
I know that I'm first of all, I'm past
my feeding window now cuz I preserve my
East Coast time feeding window. And this
is what keeps your the train running on
time. What is energy? You said energy
there. What is it?
Energy Energy is oxygen in your blood.
Everything that you perceive about
energy is nothing more than oxygen in
your blood. If you told me, "Gary, I had
a lot of energy today." Physiologically,
what you're saying is I had a lot of
oxygen in my blood today.
Oxygen equals energy.
At the start of this conversation, I
asked you a question. I said, "Why
should people listen to your message?" I
think we're now at the end of the
conversation. What have I missed that is
pertinent, important to your message
that we haven't discussed? You know, I
feel like I could talk about this
forever. Yeah, yeah, yeah. I can
imagine. Like to me, I feel like the
podcast is just getting going. Um
you know, I I I
I believe in human beings and and and
the ability of the body to heal itself.
I believe in the power of the mind and
frequency and the power of this to heal
this. Um I guess my
my message would be and I don't think
that you've missed anything. My message
would be that optimal health is found in
the basics.
Not in the complicated
fancy nootropics or some rare root
that's buried deep in the Amazon jungle.
It's found in the basics. The further we
get away from the basics, magnetism,
oxygen, light, whole foods,
the more unhealthy we become.
And you know, my message what I try to
teach on Instagram and what I the
message that I get to the world is, you
know, not that you need a lot of fancy
equipment. Sure, if you can afford it,
you can have it. But if you get back to
the basics with Mother Nature and back
to the basics with, you know, our foods,
a good
rule of thumb is if your
great-grandmother wouldn't recognize it,
don't eat it.
Um
then you'll find a state of optimal
health that's beyond
anything that you thought imaginable.
There's a superhuman inside of everybody
listening to this podcast.
Gary, we have a closing tradition on
this podcast where the last guest asks a
question for the next guest not knowing
who they're asking it for. The question
that's been left for you is, what is the
unobvious thing
that you struggle with?
Mhm.
What is the unobvious thing that I
struggle with?
You know, I
I believe that
I'm so committed to my craft
and I'm so committed to being authentic
that I struggle sometimes like everyone
else when I
I have an
extra burden of guilt whenever I want to
just have any kind of marginal
enjoyment, all right? Like if I just
want to have a cocktail or I want to eat
some birthday cake, um which I know is
not going to hurt me and it's not, um
you know, it's not going to throw me
off, but I
I really struggle with that. I feel like
I'm letting the whole world down when I
do that. Um and I know that it's not and
it's ridiculous and you shouldn't be
that, you know, being that disciplined
actually
is a you know, it's not sustainable over
over a long period of time.
Um
I think that like a lot of people
listening to this podcast, I
I'm I'm very hard on on myself. I'm my
own worst enemy sometimes.
And I have an insatiable appetite to do
what I'm doing and I think that if I
just
wasn't so hard on myself, I
probably would find it a lot easier.
Mhm.
Thank you so much. You're welcome.
Everybody listening to this should go
check out 10X Health. Um much of the
information you've discussed here lives
within that ecosystem and your Instagram
and your website and the those channels
which I've explored, you know, in in
depth are incredible resources to
understand how to start your journey to
living a more healthy life and that's
that's everything that you you espouse.
You're incredible, Gary. Thank you so
much. And you're you know, it's very
very rare that I find someone online. I
then DM them and I nagged your DM for a
couple of months to get you here. But
but I think everybody listening to this
can understand why.
You're doing incredible work and
incredibly important work in an
incredibly important time to shift the
narrative. And as I said to you I think
before we start recording or in an
interval, I I realized that this is
literally just the start for you in the
journey and the mission that you're on.
That's so clear to me. And thank you. I
feel the same way.
I've now been a Huel drinker for about 4
years roughly. So much so that I ended
up investing in the company and I play a
role on the board of the company. But
they also very kindly sponsor this
podcast. And to be honest, I've never
said this before, but Huel believed in
this podcast before anybody else. The
CEO Julian um
told me before we even launched the
podcast how successful it would be and
that Huel would back it. And I
absolutely have a huge amount of
gratitude for them for that support. But
an even greater sense of gratitude for
the fact that they've helped me stay
nutritionally complete throughout the
chaos and hecticness of my tremendously
busy business schedule. So if you
haven't tried out Huel, which I hope
most of you have at least given it a go
by now, try it out. It's an unbelievable
way to try and stay nutritionally on
course if you have a hectic busy
schedule. And let me know what you
think. Send me a tweet and a DM. Tag me.
Let me know what you think.
Interactive Summary
Ask follow-up questions or revisit key timestamps.
The video features an interview with a human biologist and mortality expert who discusses his transition from analyzing life expectancy data in the insurance industry to helping people thrive through biohacking. He argues that many chronic conditions, often accepted as consequences of aging or genetics, are actually the result of nutritional deficiencies caused by an impaired ability to process raw materials, a process known as methylation. He explains the importance of oxygen and basic natural elements, shares his work with high-profile clients like Dana White, and provides practical advice on breathwork, sunlight exposure, and cold water therapy to optimize health and extend longevity.
Suggested questions
5 ready-made promptsRecently Distilled
Videos recently processed by our community
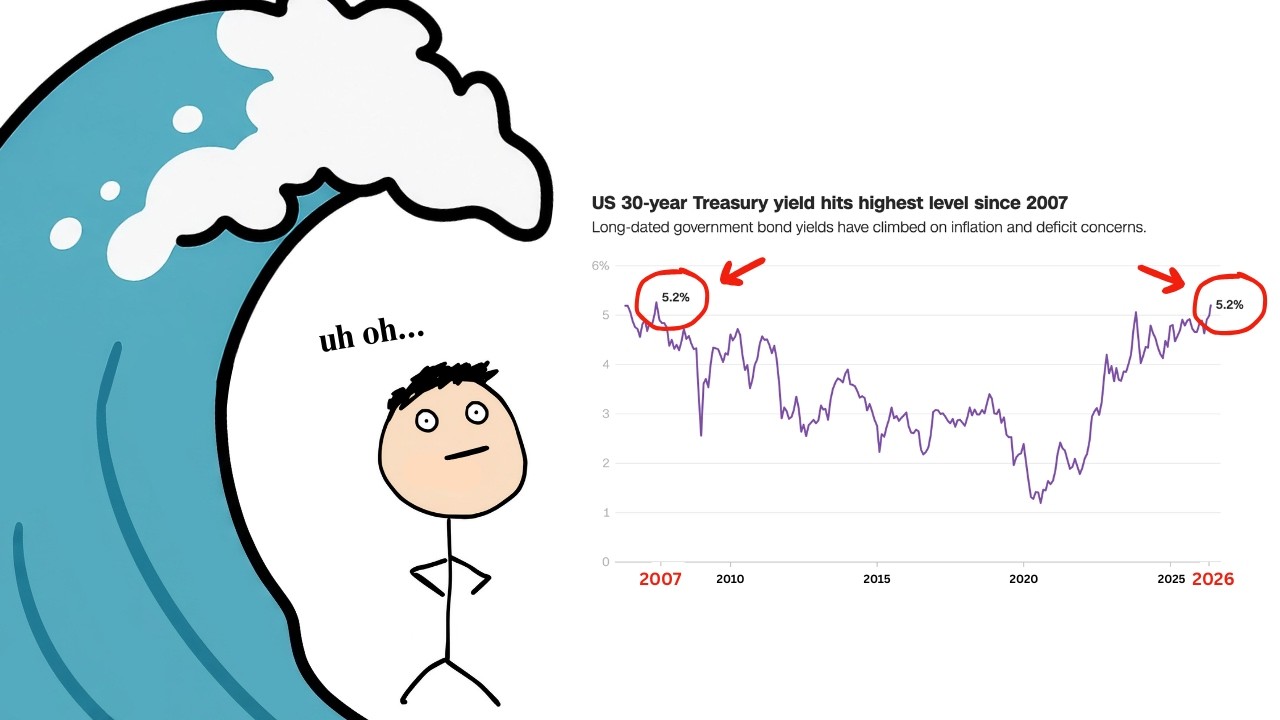
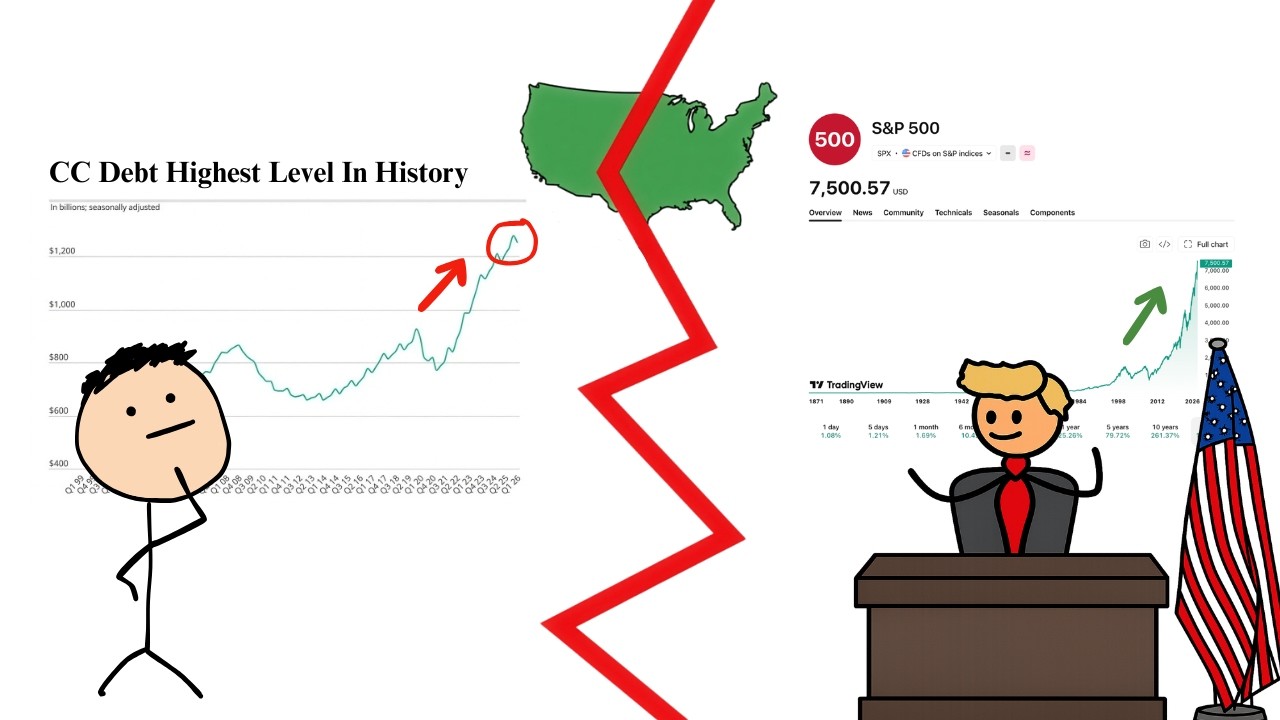

![[1hr Talk] Intro to Large Language Models](https://img.youtube.com/vi/zjkBMFhNj_g/maxresdefault.jpg)