Vitamin D Expert: The Fastest Way To Dementia & The Big Lie About Sunlight!
Now Playing
Vitamin D Expert: The Fastest Way To Dementia & The Big Lie About Sunlight!
Transcript
3693 segments
He was literally two days away from
dying. So, this is a story where a
15-year-old boy was diagnosed with blood
cancer, but he developed a flesh-eating
infection in his lung. He wasn't going
to make it. So, he has one request. He
wants to go outside, and that's exactly
what they do. And this was actually
mind-blowing to me. After the second
day, the infection is probably 60-70%
gone, and it became clear to me that
sunlight has so many important benefits.
For instance, if you're the bed closer
to the window, you get discharged from
the hospital faster. So, I want you to
give me any any information you have as
it relates to light health. For example,
do you recommend these kinds of things?
Dr. Roger Seholt is a board-certified
critical care physician who breaks down
complex science into clear, life-saving
advice. I see people at the very end of
their lives, so I know what prevents
them from getting this ill and how to
extend life. So, let's distill it down
into eight pillars. The first thing that
exercise, it reduces stroke, it reduces
depression. Next, sunlight. Did you know
that infrared lights from the sun is
able to penetrate up to about 8 mm and
stimulate and upregulate melatonin,
which prevent a lot of diseases like
dementia, cardiovascular disease,
diabetes.
>> What if you live in a cloudy country?
>> There's some very actionable things that
you can do, and we'll talk about that.
Next one, water. For instance, people
who use sauna are more likely to have
less death from cardiovascular disease.
Next, air. There are studies that show
that just going out one day a week can
elevate our immune system and make us
more relaxed. And then there's
But finally, trust. This is something
that can't be ignored because studies
have shown that people who have a good
faith and trust in a God are good.
I see messages all the time in the
comment section that some of you didn't
realize you didn't subscribe. So, if you
could do me a favor and double-check if
you're a subscriber to this channel,
that would be tremendously appreciated.
It's the simple, it's the free thing
that anybody that watches this show
frequently can do to help us here to
keep everything going in this show in
the trajectory it's on. So, please do
double check if you subscribed and uh
thank you so much because in a strange
way you are you're part of our history
and you're on this journey with us and I
appreciate you for that. So, yeah, thank
you.
Dr. Roger Schwelt.
With the work that you do, what is it
that you're aiming to accomplish?
Outside of my clinical duties, uh and
maybe even part of that, I would like to
clearly
explain
very easily graspable tools that can be
implemented to make people live their
best life and it's specifically in terms
of their health and their well-being.
And as we dig down into health and
well-being cuz that's quite a broad
Yeah.
>> basket, what is it within health and
well-being that you've spent your
career, your life focusing on? So, I'm a
board-certified internal medicine
specialist. Then I did an extra 3 years
of training uh here in the United States
on pulmonary and critical care. So, I
deal with all of the issues that are
related to the lungs and the critical
care aspect. So, if you are uh
if you were admitted to a hospital and
you're critically ill, you'd go to the
intensive care unit. I'm the doctor that
you see. So, I'm putting in, you know,
the lines, putting them on vasopressors,
intubating them. Uh I worked in the
clinic this morning.
And what are some of the unappreciated
things that most people don't think of
cuz we think of, you know, don't eat
processed food and exercise. But, is
there things outside of that that you
don't think the average person
appreciates enough? Yes, absolutely.
What are those things? So, if we look at
those things that extend life
and are beneficial, we could put them
into what I call eight pillars of
health. If you can imagine your life is
uh a chain with a bunch of links, okay?
And I'm talking medically.
Each one of those links is an organ
system.
So, your heart is a link. Your lungs are
a link. Your liver is a link. Your
kidneys, etc., etc.
As you go through life, imagine those
links starting to erode.
So that at some point in your life,
you're going to get some sort of a
disease or a diagnosis that focuses on
one organ system of your life. For many
here in the United States and in the UK,
it's the heart.
And as that link gets more eroded,
we can see very clearly that this is
going to be the link that's going to
break first. And therefore attention is
paid to that link. For many, that
diagnosis comes with medications. So
here here is where the first truism that
I would say going forward, all
medications have side effects.
And what the aim is to do in modern
medicine is to utilize the knowledge of
those medicines and their effect on the
human body so that we leverage the other
links to protect that weakest link. So I
could go through a whole bunch of
medications that I give all the time to
patients in the intensive care unit,
where I'm focused on saving their life
because I can clearly see which link is
the weakest,
but I'm doing it knowing that there's
side effects because I'm trying to save
that link to save that life. And I'm
leveraging those other things. For
instance,
somebody comes in with a stroke.
And
they have they've they've lost weakness
on the on the right side of their body
or on the left side, whichever side.
I can give them a medication
immediately that will break up all of
the clots in their body. It's called TPA
or TNK. And it will restore blood flow
to the brain and it will reverse many of
their symptoms. If they come in soon
enough, we can do this.
What's What's amazing is that that
medication has an effect that can do
that, but it also has a pretty
significant side effect in that it could
break up clots somewhere else and cause
bleeding.
So we have to be careful about what it
is that we're doing.
Clearly there, what we're doing is we're
saving one link at the expense of other
links, but that's what you have to do in
an emergency situation. But if after
that, I simply send that patient home
without telling them why they had that
stroke and what they need to do to
prevent themselves from getting that
stroke again, and what are the lifestyle
factors that caused that to happen,
I haven't done my job. So, what is what
are the interventions that we can do
hopefully early on in life
so that we don't have those links
eroding, so that all of the links are
strong, and as we get older, we can
continue to strengthen all of the links.
Here are the eight. So, nutrition.
That's That's nutrition. Basically, you
know, we know there are studies that
have done that showed that that
depending on what we put into our bodies
as food can have a dramatic impact in
terms of our well-being. Okay? So,
that's nutrition. Exercise.
As I was saying, exercise not only I
mean, drugs and things have side
effects. Exercise have side benefits.
So, exercise obviously is going to make
you more fit. It's going to make you
have better endurance.
But did you know that it reduces stroke?
Did you know that it improves
uh well-being? It reduces depression.
There's so many benefits. So, all of
these links are actually improving.
There's no leveraging here.
Exercise is incredible.
Water.
So, this may sound obvious, right? Like
you drink because you're thirsty. Where
I would like to go today is to talk a
little bit about what the effect of
water externally on your body can do.
And you're talking there about like hot
and cold
>> Exactly. usage. Exactly.
>> or cold plunges, saunas, that kind of
thing?
>> Exactly. Okay. And we'll get into the
actual evidence for this. We'll get into
it later, but what is the potential
>> system.
Which changes your probability of
diseases and stuff like that.
>> Correct. Absolutely. Especially in the
acute setting. Especially. So, not only
in the acute setting, but we also have
pretty good data from Finland, where
they have more saunas than almost than
people,
uh where they've actually done the
research and and shown with dose
response curves that this is actually
very beneficial. We won't get into too
much of that, but what I want to focus a
little bit more on because of my job in
the intensive care unit
and what we're seeing right now with
viruses and mutations and the innate
immune system, why something like this
may actually be very important, uh, as
we look forward. Interestingly, as we
look forward to future famous pandemics,
we can look backward and see what we had
done in the past. And we've got some
really actually really good information
on that. Let's go to
sunlight. This is something that, um,
I've really become more and more
involved with because of some of the
benefits that that this can do.
A very big misconception that people
have is that sunlight equals vitamin D.
And therefore, if you take a vitamin D
supplement, you don't need to go in the
sun.
This is really something that's uh, now,
um,
being debunked. Sunlight has far more
benefits than just vitamin D. Not saying
that vitamin D is is not something that
you want to supplement with. I
supplement with vitamin D. I think it's
there's a benefit to supplementing with
vitamin D, no question. But sunlight has
so many important things and I and I
really would like to spend the bulk or
the lion's share of the time talking
about this because this is really
important. Okay.
Um,
this is a this is this is amazing. Uh,
and it really made me think about
sunlight.
So, this is a story
by a lady by the name of Amy Hanmeyer.
Her 15-year-old boy
was diagnosed with lymphoblastic
leukemia, went into uh, the hospital,
actually started chemotherapy for it.
Which is blood cancer.
>> It's a blood cancer, yeah. And so, this
the treatment for blood cancer is
chemotherapy, which he started. The side
effect of chemotherapy is suppressing
the immune system.
And unfortunately, he didn't realize it,
but he developed uh, he didn't realize
it immediately, but he developed a a
fungus flesh-eating infection in his
lung.
And went into the hospital in June of
2024.
Uh this is in Minnesota, tertiary care
hospital.
And he
got worse and got worse and got worse to
the point where the only way that they
could control this infection was to
actually remove his left lung, which
they did.
So, this is a 15-year-old boy.
He is without his left lung. He only has
a right lung.
And he starts to decline even after
that. They do a CT scan and it shows
that now the infection has moved to the
his remaining right lung.
They have a family conference.
And as Amy is telling me this story, I
could hear her choking up. She's telling
me this on the phone.
She's saying that he's 15, he's
completely awake, he's completely alert.
He knows everything that's going on
around him. He's on a ventilator like a
a machine that they use for for sleep
apnea. It's like a BiPAP machine that's
breathing for him. It's not intubation,
but it's on his on his mouth.
And the doctors, you know, have done
everything they possibly can and they
say, "Look, he's getting worse. We can't
take Obviously, we can't take the right
lung out. We can't put him on a
heart-lung machine because there's no
sort of destination to where he's
going."
Uh
we recommend not intubating him and
making him what they call DNR, do not
resuscitate.
So, they're like, "Wow." They were not
expecting this coming. So, they have a
big conference. Somebody they they call
in help to like, "How do you explain to
a 15-year-old boy that you're dying?
And how how's that going to feel?"
So, they asked the doctors, "How how
much time does he have?" They say, "2
days."
So,
in this in this situation,
they ask this boy,
"Okay, you're going to die.
What do you want to do with your life in
the in the next 2 days? What do you want
to do?
And surprisingly, he says, "I want to go
outside."
"I just want to go outside."
This this guy grew up probably on a farm
or something and he spent his time
outside. So, he wants to go outside.
So, you know how
I mean, I don't know if you know this,
but like if you're a nurse or you're a
doctor
and you've done everything you can and
this and you're just completely
horrified at the fact that this
15-year-old is going to die and he has
one request, you're going to move heaven
and earth
to fulfill that one request. And that's
exactly what they do. They
get this boy the hospital bed outside.
He's on a BiPAP machine the respiratory
therapists have put together. So, this
guy is outside.
And they're not putting him outside to
get better.
He's just this is his dying wish. They
also use this thing called a Firefly.
It's like a a light device that they
were using. I to I'll be honest, I don't
know which did it. The Firefly was the
It's a It's a light device that gives
off light at different wavelengths and
they would use that for about three
times a day for 5 minutes.
This guy
does not die.
After the first day
his white count starts to come down.
That's like a a measure of the infection
that's going on in the lung.
And and and by the way, they do a CT
scan of his lung before this all starts
and the and it's just the the the
remaining lung on the right is just
filled with infection. It's horrible.
By the By the second day, the white
count comes down even more. And and by
the way, they haven't changed any of the
other treatment. He's been in By this
point, he's been in for 6 weeks.
He has not seen the light of day.
And and he's still getting the powerful
antifungal medication amphotericin B and
posaconazole. All of these things are
are really high-powered drugs that that
just completely fight fungus, but it's
not working. He's getting worse.
But now, he's out for the second day.
The white count's coming down, which is
good. That's a good sign.
His oxygen requirement is coming down.
That's a good sign. He's requiring less
and less oxygen. By the time he gets to
day five,
okay, we're already past two days.
He's off the BiPAP. He's on regular
just nasal cannula oxygen that you see
people wearing on their nose.
The doctors are scratching their head.
They're like, we we should get a CT scan
to see what's going on.
So So, Amy tells me that they they get a
CT scan of this guy, and they're in the
room. And some some even like swear
under their breath. Like they they're
completely
amazed.
Because on the CT scan, obviously the
left lung is still gone.
But the right lung,
the disease is probably 60 70% gone. And
he he's still alive.
He goes home. There's no sign of the
disease after after treatment. And he he
uh I I just she just uh communicated
with me to tell me that he just got his
Make-A-Wish
uh thing for for his cancer. He's
continuing treatment.
And to And she just can't believe that
he was literally two day two days away
from dying.
They changed nothing. They changed none
of his treatments. The only thing that
they did was they took him outside and
they they were using this Firefly before
inside, but they were using it more
consistently when he got outside.
Maybe hospitals should be outside.
>> This is exactly what
Okay, so if you wanted to know what my
drive was, what what it is my purpose
that I'm doing right now, I'm working at
three different hospitals. And
I'm trying to work in each of those
three different hospitals to try to get
patients outside. The biggest barrier
that we have is staff taking those
patients outside. That's the thing
that's the hardest. But this is what we
used to do.
Steven, this is what we used
When we built hospitals at the turn of
the century, we had hospital rooms where
beds could be taken out onto the veranda
and people could get sunlight. I would
love to see a time where we could go
back to that type of effect. There are
studies that have been done. People in a
two-bed room,
if you're the bed closer to the window,
you get discharged from the hospital
faster, on average.
Really? Yes.
I need to swap sides of the bed with my
girlfriend.
She's on the sunny side.
>> There There's so much evidence for this.
People who are in hospitals that are
have bigger windows, they give better
surveys.
And hospitals
reimbursement is tied
to the surveys that they get from
patients. So, it's literally a
win-win-win. If hospitals started to, I
believe, get patients outside. And And
they're already doing this. There
I don't want to say that this isn't
happening. There are hospitals that are
have programs to get patients outside.
Um I think we just ought to be doing it
a lot more.
Um
temperance. Temperance? What does that
mean?
>> It's an old term, isn't it? It really
means
moderation. And And I I would say in
this sense, temperance really means to
avoid toxins in the body.
Um As somebody who is a pulmonologist,
who is What's a pulmonologist?
>> is someone who takes care of the lungs.
And so, as a result of that, I see a lot
of issues with lung cancer
related to smoking.
Um I see it in the intensive care unit,
people with liver failure as result of
alcohol abuse. I also see people
on amphetamines. Here in Southern
California, where I reside and where I
work, we we have quite a bit of that.
And uh temperance, if if you want to
live a long and wholesome life, there
are some toxins that you want to avoid.
And uh And And And understanding that is
really important. So, this is something
that, if you stop some of those things
that we're talking about, all of those
links are going to be improved.
Air.
Seems kind of obvious. Early on I used
to think that that what this meant was
getting pure air with absolutely nothing
in it except for just nitrogen and
oxygen.
That's not true anymore.
We now understand that for you to have
the best type of air,
it actually has to come with some things
in it. Just like our our gut has a
microflora that you may have heard
about, so too does the air that we
breathe also must have that. And the
best type of air that you can have is
actually outside.
Rest.
This is really interesting because we
just mentioned that exercise was a
pillar, but rest also is. How can rest
and exercise at the same time be pillars
of health? And it really comes down to
knowing when to do what. Sleep, which is
also part of rest. So we're not just
talking about a daily rest when you go
to sleep. And and as a sleep physician I
can tell you quite a bit. We have lots
of information about how long we should
sleep, the quality of sleep, some of the
diseases that prevent us from sleeping.
Sleep is so important. I can't I I
couldn't over express it enough. Not
just a a daily rest, but I would also
say and and venture out we can talk more
about this, a weekly rest. A weekly
rest?
>> A weekly rest.
What do you mean weekend? Yeah. Yeah,
absolutely. How many times do we even on
the weekend do we put down our our
phone? Never. Or we stop reading emails.
And we take the time out to do things
that we would never be able to do.
Finally, trust.
So this is something that really just
can't be ignored. And and I'll say this
up front that um
in the world of research and science
there is a there is a silo of science
and there is a silo of faith. But,
what's what we can't ignore is the
growing body of evidence
from the scientific world that's peeking
over and looking at faith, that people
who have faith and people who have faith
in God,
uh whether that is uh their God in in
that particular denomination, are better
apt and able to deal with stress and
depression and anxiety.
So, this is something scientifically
that has been shown. Now,
if you you may have noticed that I I did
these in a particular order.
Um and if you go through them, you've
got nutrition,
you've got exercise, you've got water,
you've got sunlight, you've got
temperance, you have air, you have rest,
and finally you have trust. You put that
together and it spells out NEWSTART.
So, interestingly, these these
particular topics are not copyrighted,
but there is a um there is a university
in Northern California called Weimar
University that has actually put these
together in that very pattern as called
it NEWSTART. They actually have a
NEWSTART program.
Um and so, this is something that uh
that is actually being used uh
internationally.
So, of these subjects that you just went
through there for this NEWSTART um
framework,
where do you want to start?
I think actually sunlight is is one of
those things where I'm excited about all
of those, but I think sunlight is
is really where we have It's the Let's
put it this way, it's the lowest-hanging
fruit. Okay. Explain to me why sunlight
is the the place where your focus is at
the moment.
It's a long trip that has gotten me to
that. Um and I and I think part of it
has to has goes through right through
COVID.
So, as a critical care intensivist, when
I heard that there was this virus that
was coming, they all told us that it was
going to be people with respiratory
illnesses, which I was certainly
comfortable with.
But, that's not what it turned out to
be. We certainly saw people with
respiratory illnesses, but what we saw
in the intensive care unit, the people
that were dying around me
were people with obesity, people with
heart disease, people with kidney
disease, people with dementia, people
with chronic diseases.
And it made me think, why was that the
case?
All of those things
have one thing in common.
And many other things, too. But,
specifically, they're rooted in
something called mitochondrial
dysfunction. So, let me unpack that for
you.
And and this has to do with longevity,
this has to do with aging. This is a
huge topic that is now just emerging.
And we're we're now finding more about
this. So, what when we were when I was
in high school biology, when I was in
college, uh we all learned about this
little organelle in all of our cells,
except for red blood cells, called the
mitochondria. And and and I have to say
it, what is the mitochondria? It's the
powerhouse of the cell, right? So, it's
the thing that makes energy.
What we didn't know at the time is that
as we get older, the output from these
batteries in our cells drops by about
70%. Damn. Can you imagine running your
house on 70% less energy? Well, how
fundamentally that would change what
change what happens in your house? Like,
you could not run the laundry the same
way. You could not run the microwave and
the laundry at the same time.
>> And what does that look like in terms of
symptoms? Excellent question, because
what it looks like is depending on the
cell type that we're talking about,
that's going to have the issue. So, if
we're talking about the liver, the
liver's going to get more fatty. If
we're talking about the heart, the
heart's going to is going to become more
congested. If we're talking about the
brain, it's going to have more dementia.
And so, what's what's happening here is
that as we get older, the batteries in
our cells are not working the same way
as they used to. Metabolism is slowing
down.
And and so, these are these are huge
issues.
And all of these diseases that I just
talked about, all the ones that we saw
in COVID, if you look in a lot of these
diseases, they are rooted in
mitochondrial dysfunction. So, the
question is is why is that the case and
what can we do about it?
So, there was a paper that came out in
2019
that fundamentally changed the way I saw
this. It was written by Russell Reiter
who is the
executive editor of melatonin research.
It's a he's out of University of Texas.
And Scott Zimmerman who's a light
engineer. And what they set forth was to
show that basically
sunlight
is
made up of so many different types of
wavelengths. You've got ultraviolet on
one end which of course makes vitamin D.
And it's very beneficial. It it it's the
type of light from the from the sun that
is very short wave
and but cannot penetrate very deeply.
Let let me let me back up a little bit
and explain.
You pull up to a stop sign and somebody
pulls up next to you and they're playing
the latest hip-hop music. How does that
sound to you in your car?
It's very boom boom, right?
>> Yeah, muffled. It muffled. And the
reason why is because low wave frequency
has the ability to travel very far.
Go to the Grand Canyon and there's a
thunderstorm at the other end of it.
What do you hear? It's like a rumbling.
And then as it gets closer, you hear the
higher pitched sounds. This is a
fundamental physics
principle. And so when the sun is is
shining, there's very short wavelengths,
ultraviolet B involved in vitamin D. But
at the other end, there's this infrared
light which we'll talk about or red
light. It's very long wavelength and it
can penetrate very very deeply.
That's very important because what we're
talking about is the human body. And if
the sun is going to have an effect on
the human body, it's got to be more than
just the skin.
So, that's exactly what what this paper
showed is that basically
infrared lights
from the sun
is able to penetrate probably up to
about 8 cm according to Scott Zimmerman
in this article.
And it fundamentally interacts with
specifically the mitochondria.
And what does it do to the mitochondria?
So let's let's back up and talk about
the mitochondria cuz this is central.
The mitochondria to the cell is like the
engine in your car.
The engine produces locomotion that
causes this the wheels to spin. But in
the process of doing it
it causes heat to surround the engine.
And if you don't deal with that heat
it will shut down the engine. It will
make it more inefficient and eventually
it will shut it down. So what do all
internal combustion engines have? They
have a cooling system. They have a
radiator. They have a an oil pan. They
have a water pump. And that's exactly
what the cell has to have for the
mitochondria. It's not heat in the
mitochondria. It's called oxidative
stress. And it's specifically oxidative
stress that causes destruction and
and yeah, destruction of the
mitochondria and leads to these types of
diseases. So oxidative stress causes the
mitochondria not to work well. This
leads to diabetes. Oxidative stress
makes the mitochondria not work so well.
This leads to dementia. So there's a
This has already been laid out. This is
not that controversial. The
controversial part is what do we do
about it? So what these guys in this
paper showed
was that and and not just them but look
reviewing the literature is that the
mitochondria makes its own cooling
system.
And that cooling system is melatonin.
Now you might think be thinking, wait a
minute, melatonin, isn't that the isn't
that the stuff that we take that our
brain makes right before we go to sleep?
Yeah, that you're it's absolutely
correct. That's what happens.
The problem is is that this is not
melatonin that's made in the brain. This
is not melatonin that goes through the
blood supply and goes to It through our
blood and tells us it's time to go to
sleep. This is melatonin that's made in
the cell in the mitochondria.
And it's a powerful antioxidant that
basically prevents the oxidative stress
from occurring.
What Scott Zimmerman and Russell Reiter
showed and and proposed in this was that
basically the infrared radiation that's
coming in
to the body is able to stimulate and
upregulate melatonin and a number of
other factors that keep the mitochondria
cool and can actually improve the energy
output of the mitochondria.
So this is This was actually
mind-blowing to me and I'll tell you why
I resonated with this as a critical care
physician because there was two things
that bothered me the most. Number one.
SARS-CoV-2 virus. When it comes into the
body, it interacts with something called
the ACE2 receptor. You may have heard
about the ACE2 receptor. Okay. This is
where the the virus actually latches on
to the cell
and gets internalized. So what is this
ACE2 receptor? Is this Was this there
for all of humanity just to be a
receptor or does it actually have a
role?
It turns out it actually has a role and
mind-blowingly
the ACE2 receptor is involved in
mitigating oxidative stress.
So in other words, it's another part of
the cell's cooling system for the
mitochondria.
What
what's happening is that the
the virus when it attaches to the cell
is basically eliminating that action.
And so
imagine you have a bunch of people with
various different engines running at
different temperatures. In other words,
you've got some people with chronic
disease and we know their engines are
running hot. We have some other people
who are completely healthy and they're
doing quite well. Their engines are nice
and cool. They have no problems at all.
Now imagine COVID comes and SARS-CoV-2
is infecting everybody.
What that tendency is to do is because
it's knocking out everybody's ACE2
receptor, which has the ability to cool
down the engine if in other words, it's
causing everybody's engine to run hot.
Right? So, but in somebody So, in other
words, picture it this way. You're
You're You're driving along in your car
and your thermometer is there and all of
a sudden there's this big hill that you
have to climb, called COVID-19. Who's
going to make it over that hill and
who's not going to make it over that
hill?
The people that make it over the hill
are those with great cooling engines
that whose temperatures are running
great. The ones that don't make it over
that hill are the ones that have the
thermometer on their engine running hot.
Those are the ones that poop out at the
top and can't make it and they're
they're the ones pulled over to the side
of the road with the hood up and the
steam coming out of the out of the
engine. Do you understand what I'm
saying?
>> yeah. So, this makes perfect sense to me
why I wasn't seeing what they were
predicting, which is respiratory
patients coming into the ICU. Who was I
seeing in the ICU? I was seeing people
with dementias, as we talked about,
diabetes, kidney disease. These are the
ones that were that that were sick. The
other thing that that really hit me
and resonated with this
was and this was this was not even
controversial. We knew early on in the
pandemic that people who came into the
hospital and had higher levels of
vitamin D
did really well.
They didn't die.
They They didn't have the same chances
of dying. People who had low vitamin D
levels, they had much higher levels
chances of dying.
So, we would check these vitamin D
levels. And so,
think about this. You're You're there at
ground zero and you're taking care of
these patients and you see this data
over and over and over again that
vitamin D is very predictive of who's
going to die. Obviously, what are you
going to do? Even though this is an
associative study, that association
doesn't mean causation, you're going to
be giving people vitamin D
and try to get those levels up.
The problem is is that we gave vitamin D
and it really didn't have much of an
effect.
So, you gave it in supplement tablets.
>> Yeah, when people would come into the
hospital exactly.
Exactly, just like that. In fact, I was
supplementing myself. I mean, what have
you got to lose, right?
I already took my vitamin D tablet this
morning. I don't There's not There's
very hard to overdose, but it's
possible. So, you noticed that it was
hard to treat people with vitamin D, but
giving them a a tablet didn't really do
much. That's correct. Why?
Well, this is what I believe is the is
the is the fact is we saw that people
with high levels of vitamin D or normal
levels of vitamin D did better than
those that had low levels. I believe
that that was a marker of something
else.
In other words, people who had higher
levels of vitamin D meant
that they were out in the sun more. They
were outside more.
Than those the people that had very low
vitamin D levels. The people with low
vitamin D levels were telling me these
are people that were not getting outside
into the sun. And so, what's the real
factor here? What's doing the heavy
lifting? And I would propose and Scott
Zimmerman and Russell Reiter would
propose, and I can tell you a number of
other scientists that would agree with
me on this,
is that infrared radiation
from the sun
is causing an effect at the
mitochondrial level in terms of
oxidative stress.
And that vitamin D was just the marker
of who was getting the infrared light
and who was not. Who was going outside
and who was not going outside. So, when
the sun is shining for the most part,
you're getting infrared light. You're
getting the entire the entire biological
spectrum from the sun. We can go to the
longest wavelength, which is far
infrared,
all the way to the shortest wavelength,
which is ultraviolet B, okay, which
makes vitamin D.
So, in other words, when you are outside
in a natural environment, you're getting
a very broad spectrum of light.
And so, because of that, if you're
getting infrared light, you're also
going to be making vitamin D.
Yeah, you're getting both.
Um
Now, that can change because in the
wintertime
when the sun is lower in the sky,
especially, you know, in England, this
is this is a special issue at that
latitude. When the sun is low in the
sky, it's got the light has to penetrate
through obliquely through the
atmosphere. And because of that,
shortwave
radiation from the sun, like ultraviolet
B, does not make it very well. So,
there's times of the year where you're
not getting enough ultraviolet B or
maybe even no ultraviolet B from the
sun. Which makes the vitamin D. Which
makes the vitamin D. And that you're
you're going to be deficient, you need
to supplement. However,
during that same period of time
when you're not getting enough vitamin D
because there's no ultraviolet B
radiation, that sun is low, but that's
it's still enough to allow that long
wavelength penetrating infrared light to
still come through. So, is the longwave
infrared light the type of thing that we
see
these gadgets doing? Absolutely. And and
I would say just to be specific is
because you can see that as red light
there, that's not infrared light because
you can see it.
So, infrared light technically is
completely invisible. But this these do
give out infrared light, but you just
can't see it.
>> So, it's toward that red end of the
spectrum. And people like Glen Jeffery
out of UCL
is actually doing research at 670
nanometers of red light and has shown
in randomized controlled trials that
that type of light right there at 670,
the type that you can even see,
actually does improve mitochondrial
efficiency. He's shown this in a number
of randomized controlled trials. It
improves eyesight. And and you have to
realize that the retina at the back of
your eye is very rich in mitochondria.
He's shown this in terms of managing
glucose and and output for mitochondria.
And and the reason why these things work
so well is because what's going on here
is as you get older, your skin starts to
become more saggy because the the
fibroblast or the cells in your skin,
they're designed to make collagen and
collagen is the skeleton that makes your
skin soft and subtle. Yeah. Don't mind
me. Please carry
>> No, no. So this is this is exactly My
wife uses the same thing. This is a fun
charge one day.
>> So what what's going on right now is
that red light
which can penetrate very deeply down is
going into the skin and it is activating
the mitochondria in your fibroblast to
produce more energy which those cells
need to deposit collagen. And so when
you deposit collagen, that's going to
give the skin a more tight uh feel
because as you get older, that collagen
deposition is going to get less and less
and less.
>> So this is going to help keep me looking
young. That's the whole point of it. And
you're saying that the the light in
these penetrates what, 6 or 7 cm or is
it
>> does about 8 cm. Uh this red light would
be a little bit less because this
light obviously you can see it, so it is
a little bit shorter wavelength, but
yes, this light, the red light can
penetrate deeper than for instance
yellow light or blue light. And it's
this light particularly that interacts
with the mitochondria to increase that.
So should we be putting this all over
our body because okay, it's good for my
skin, but if it's penetrating deeper,
presumably those other parts of my body
that would benefit from that, another
mitochondria. It's interesting you say
that. Um the the the study that I'm
referring to with Glenn Jeffery out of
University College London, he took uh
young people in this study. He gave them
a a bunch of glucose. And everybody who
gets a bunch of glucose should have a
spike in their blood sugar.
And he randomized them on their backs
to see what would happen when he shined
red lights uh on their backs. And the
people that got the red light had lower
spikes. In other words, it seemed as
though the mitochondria
were metabolizing faster, which caused
less of a spike of the glucose in their
blood. The way he confirmed that is
looking for the byproducts of the
mitochondrial metabolism, which is
carbon dioxide. So, when we breathe,
when we metabolize, we're breathing out
carbon dioxide, which is the result of
of a mitochondrial metabolism. And in
fact, in those people that had the light
on,
it showed a higher level of carbon
dioxide in the exhaled breath. The whole
point of that is to get back to your
question is whether we should putting
this all over your body. He was able to
get that effect systemically with just
putting the light on the back.
Um that was a that was a systemic
ability. What We don't understand
everything about the mitochondria, but
what we do seem to understand is that
they can communicate with each other.
And that you don't need to have this all
over the body to have systemic effects.
In this particular case though, if you
want to have the skin here to be more
you know, younger-looking, then it makes
sense that this is where you need to
have it. If you want to have a
particular other part of your body to
look younger, then then perhaps that
that's where the light needs to go. So
interesting. So how long did it take in
those studies to see the effect of red
light therapy like this? Well, that's a
very good question. If you talk to Glenn
Jeffery, which I have, he noticed a an
improvement in 15 minutes.
15 15 minutes? What did he notice in 15
minutes? He said he has studied the
mitochondria in fruit flies and in
mosquitoes and bees and in human beings
and it's the same every time. He says
after about 15 to 20 minutes of this
type of light in that type of setting,
there is a switch
that turns on and it and you and you
don't need further stimulation. Further
stimulation doesn't do anything more.
It's a it's a very bizarre thing. You
would think that the more light that you
gave, the more the effect would be. It's
not. After about 15 minutes, it it
there's something that changes in the
mitochondria.
There are certain theories about where
this might be. This might be in the
electron transport chain
complex four. Uh these are very
technical things. There's a lot of
studies that are actually There's a
number of groups that are actually
looking at this.
Uh there's a whole area of science
called photobiomodulation, which is
looking at this. But, 15 minutes is
really what it takes. So, we're not
we're not talking about a long period of
time.
This is really really interesting. So,
getting back to my
experience in the intensive care unit.
The vitamin D wasn't working.
These patients were dying, and it became
clear to me that COVID was a metabolic
issue
for these patients.
By the time I had realized this,
the sir I mean, the pandemic arguably is
still going on because people are still
becoming infected, but the rush to come
into the hospital and the and the number
of bodies that we were seeing
circulating through the intensive care
unit had dropped dramatically.
And at that point, I was able to
see that potentially
infrared lights may be very beneficial
in these patients with COVID-19. Now,
there was a study in Brazil. They took
COVID patients
that were that were sick enough to be
admitted to the hospital, but not too
sick to be intubated in intensive care
unit.
And they did something tremendous. They
actually manufactured a jacket that they
could put on patients. And on the inside
of this jacket were these LED bulbs that
gave off
infrared radiation at exactly 940
nanometers. They put the jackets on,
and they randomly randomized assign
which jacket was turned on and which
jacket was turned off. It was blinded
because the light coming from this
jacket could not be seen by the human
eye. It wasn't even enough to produce
enough heat.
And so they they did this on 30 subjects
and they randomized them. 15 did it 50
50 all 15 had or all 30 had the jackets
on. 15 had it turned on, 15 did not have
it turned on. And they watched them.
What happens to these patients?
Every single endpoint that they looked
at was statistically significant.
And What does that mean?
>> It means that the differences between
these two groups could not have been
from chance.
There was a real difference.
The group that had the jacket turned on
had improvement in their oxygen
saturation.
Had could take breaths in more deeply
and stronger. Had improvements in their
blood white blood cells.
Um and not only that, had improvements
in their heart rate, their respiratory
rate, all of these statistically
significant. But the most important and
mind-blowing statistic was the length of
stay in the hospital.
So,
they had these jackets on
for 15 minutes
once a day
for 7 days.
In the group that did not have the
jacket turned on, their average length
of stay was 12 days in the hospital.
For those that had the jacket turned on,
it was eight days. That was four day
difference. That's tremendous when you
realize that it costs thousands of
dollars
to hospitalize patients.
It's it's a huge amount when you think
about the fact that there are certain
drugs that get FDA approved for
influenza for instance by just cutting
short the symptoms for 24 hours. This is
not just 24 hours for people were
discharged
from the hospital four days faster. When
I saw that study, that was enough for me
to convince me. I mean obviously it was
30 subjects, right? We should do a
bigger study. We should do a hundred a
couple hundred, right? That would be
that would be ideal to do. But the fact
that with just 30 patients they could
show statistical significance. That was
enough for me to say every patient from
now on that I see
that comes in with COVID-19 that's
hospitalized, that they're asking me to
go intubate, to bring to my ICU, these
patients are going to get outside.
I don't have that jacket that they made
in Brazil.
I I I don't even know how I would make
that jacket. They made it for the study.
And it's not commercially available.
There's no 940 nanometer lights, which
is what they did in the study. But I do
know this. I do know that sunlight has
940 nanometers in it.
And if I could just take these patients
outside
maybe they could improve. So I had I got
my wish.
I had a patient on the floor.
He was on 35 liters a minute.
100% oxygen through high flow. Through
his nose. Through his nose. Barely
barely saturating because he had
COVID-19.
And uh I was asked to go see him because
he was potentially needing to be
intubated or brought to the intensive
care unit. I could not believe it cuz I
had not seen one of these in months. So
I went down, walked into the room,
opened the door. It was in isolation. I
had a mask on, the whole nine yards. The
room was completely dark. The blind was
closed. His daughter was there. And the
first words out of his mouth to me was
"Doc, how much time have I got?"
I mean, it was a catastrophe. Like
there's no light, no circadian rhythm.
This guy was depressed.
I immediately called my respiratory
therapist, immediately called the charge
nurse. We got everybody together. And I
said, "We need to get this guy outside."
It was a bright and sunny day.
How are we going to get this guy
outside? 35 liters, 100%. We My
respiratory therapist, Kim, managed to
put a couple of oxygen tanks together.
And we were able to get this guy into a
wheelchair.
And we wheeled him outside.
And uh he told me this uh weeks later.
But he says, "You know, that first day
that you got me outside in the sun cuz
we did this for like 7 days in a row.
He said, "That felt so good."
Um he after just 1 day dropped down from
35 L to 15 L.
15 L of of oxygen. And then down to 12,
and then down to 8 the next day, and
then down to 5. 5 days The amount of
oxygen he was inhaling to keep him
alive. Correct. So, in other words, we
were titrating down the amount of oxygen
that we had to give him to maintain a
saturation in the 90s. In 5 days he was
discharged home without oxygen.
Now, obviously that's an anecdote,
right? That's not a study. But, I'm
looking at the risks of getting people
out in the sun for 15-20 minutes.
There's not a lot of risk to that. And
if there's a benefit, I thought it was
worthwhile doing. We we need to have
larger randomized controlled trials, but
it got me down the road to looking to
see what what was it
about sunlight
that was affecting this change. And you
know what? There was There's There's
ample data.
There There was a study actually that
was done
in in Europe where they looked They
said, "Okay, here's COVID. COVID's going
up. When does COVID go up? Is it because
of temperature that changes? Is it
because of humidity?" And the answers to
both of those were no. Do you know what
predicted when countries were to have
their first surge in the autumn of 2020?
There was a study that was actually done
on this.
It was latitude.
It started in Finland
and then real it went down the entire
continent. The last country in the in
the autumn of 2020 to have a COVID surge
was Greece.
So, as the sun is literally pulling down
into the southern hemisphere, as the
shadow starts to go over Europe, that's
when we start to see
COVID surges one by one by one. There
was Yeah. Is that Is that because COVID
and the sun aren't friends? So, if I it
makes it harder to spread because, you
know, if I put COVID on this table and
then I put sunlight on the table, the
COVID is going to die. Yeah, it's
possible. Although we now know that
COVID probably doesn't spread too much
through contact. It's it's more of an
airborne thing. So there there was a
study that was done at the University of
Edinburgh.
And they looked at this very question
that we had talked about earlier about
vitamin D. They looked at the United
States in the in the wintertime.
So and they eliminated the southern part
of the United States because in the
southern part of the United States you
can actually get some vitamin D in the
wintertime. So they just looked at the
sort of the northern portion of the
United States and they were able to show
that the more sunlight there was in
particular areas, the lower the
mortality from COVID-19.
So they said, "Well, this is
interesting.
What about in England?" So they they did
the exact same study in England and and
sure enough of course they didn't have
to eliminate any part of England because
the whole country doesn't get in any
vitamin D in the wintertime. What they
showed was that again, certain parts of
the country in England as you know, get
more sunlight than other parts. Well,
those areas that got more sunlight had
lower
mortality from COVID-19. Then they took
the same
They predicated the same study and they
looked in Italy.
Exactly the same finding and they
published this. And they said in their
study and this is what really amazed me.
They said,
"The fact if this is causal,
they say." They said that
this might actually show a possible
public health intervention. The fact
that it is completely independent of
vitamin D means that there's something
else going on.
There was a study in 2011 in Sweden.
Yes.
Is that linked to this?
>> No, this is a completely different
study. But that that's also a very
important study. So the Swedish study is
is is groundbreaking. Um
This was a study where they asked 20,000
20 to 30,000 Swedish women
about their habits in sunlight.
And they divided these women into three
categories. Those women that did not get
a lot of sun, those that got a moderate
amount of sun, and those that got a lot
of sun. And they followed them for 20
years. And they they kept a track of
each one that died and what they died
of.
And when they were done with that, they
were astonished because what they found
was that
the women who had spent most spent the
large amount of their time outside or
that spent the most amount of time
outside
had
the least amount of mortality from
cancer,
from cardiovascular disease, and
non-cardiovascular disease. And those
that spent the least amount of time
outside had the highest levels of that.
The magnitude difference between those
two was so much
that they were able to show that women
who in Sweden
who spent the most amount of time
outside and smoked
had the same mortality as those women
that did not spend as much time outside
and did not smoke.
They were equal. They were equal. In
other words,
being in that category of not spending
much time outside in the sun was the
same risk factor for death as smoking.
How do they know it wasn't linked to
exercise? How are they able to establish
causation cuz that's a You're absolutely
That's an excellent question. So, the
the difference here as you go up is this
is a this is an association study, okay?
So, the question is is how can you get
causation from association? You can't.
But, if you look at the Bradford Hill
criteria, there is a way that you can
potentially make a a strong argument for
causation if there's something called a
dose-response curve. In other words, if
you can show you're not just comparing
two things, but you're comparing three
or more, if you can show that as you
increase
the variable, that there is a change in
the
the outputs that is strongly suggestive
of potentially causation. By the way,
this is exactly what we did to show that
smoking causes lung cancer. Obviously,
we can't do a randomized control trial
here. You get to smoke, you don't get to
smoke. We'll follow up in 20 years to
see who has lung cancer. This is exactly
what we did. We showed that that there
was such a strong association with
cancer risk with smoking that we were
able to say through association that
smoking causes lung cancer. By the way,
Richard Weller
was a dermatologist in England uh did
just last year a very similar study as
to the Swedish study except it was 10
times bigger
and he did it with both men and women.
He found the same results.
It was a UK Biobank study.
What did he discover? He discovered that
either from
from solariums or from um or being
outside using solar radiation data
uh he was able to show both on their
their questionnaire and also where they
lived
that the more light that they had the
lower their risk as of of um mortality
uh and um and cancer mortality. So, the
question was
does it increase melanoma?
What's melanoma? Melanoma is is a skin
cancer. So, that's the big risk. That's
the big risk that everybody's concerned
about. You go out into the sun sun and
you're going to get skin cancer.
And he was able to show in that study
this was like three three 400,000 people
in this study. UK Biobank study, Richard
Weller.
He was able to show that
there was no increased there's no
statistical increased risk of melanoma
incidence but there was
a reduction in non-skin cancer
mortality.
Okay, so so here's the trade-off. If you
want to go out into the sun in England
okay?
The benefits are you're going to have a
reduction
in non-skin cancer mortality. So,
everything other than skin cancer?
>> Correct.
On the other hand, there's no increase
in melanoma incidence. So, that caused
him to write an a an op-ed and publish
it. And actually, you can look up this
op-ed. It's a great op-ed. Uh it
published in a um
in the Journal of Investigative
Dermatology called Sunlight: Time for a
Rethink. Where he goes through the
arguments. And he's actually shown And
there's been a number of changes that
people have making around the globe. So,
public health uh
organizations that are saying now, you
know, before we have said
that, you know, the the sun is a deadly
laser.
And you should avoid it at all costs.
We may need to rethink that.
So, you telling me that essentially 15
minutes in the sun every day turns on a
switch in my body that improves my
mitochondrial function, which is going
to impact a variety of different parts
of my health. Is that essentially what
you're saying? Essentially, yes. Uh and
and we're we're looking And this is in
an environment where where we are
spending less and less and less time.
To give To give you To put in
perspective, if we were on a British
ship 300 years ago, and I came to you
and I said, "Do you see this little
yellow fruit? Just by eating a little
bit of this yellow fruit, all of this
disease that you're seeing around you
with your fellow shipmates is going to
go away." That that would seem almost
incredulous, right? But, that's exactly
the case.
We We are
The scurvy of the 21st century is the
lack of sunlight.
Everything is inside.
Uh we we avoid the outside. We avoid
discomfort. We avoid high temperatures.
We avoid low temperatures. We uh are We
used to go out and play sports. We now
are are playing virtual sports on on
pads.
We have windows
that are specifically designed,
especially here here Southern
California, to eliminate infrared
lights. Because why? Infrared lights
comes in and it heats up. One of the
interesting things we didn't mention
this about infrared light is the way
that we interact with infrared light.
You can You can tell this on your own.
You go outside
and
close your eyes. You can tell which side
of your body the sun is on. And the
reason is is because that infrared light
not only can penetrate through your
body, it's also penetrating through
clothes
very easily.
And you can feel that. That That heat
that you're feeling is the infrared
light going through this going through
the clothes, going through the skin, and
interacting with your heat receptors
that are well below the surface.
Um so all of this
All right, guys. Pretty good. I got
Steve. The guest is here.
Ready? Come in. OH MY GOD, STEVE.
LOOK.
WE DID IT. THIS IS a the Boncharge face
mask. It's good for blemishes, wrinkles.
Uh clears up the skin. It's red light.
Have you not used it before? No. You
tried this before? It's um
It's really, really good. It shines red
light on your face, which helps increase
and boost collagen production. I
actually found it out cuz of the missus.
Seeing her wearing it, she terrified me
a couple of nights in a row. Um I
thought it was to scare people with, but
actually it's really, really good for
your skin. So
they are a sponsor of the podcast and uh
I've been using it every day for about a
year and a half now.
You're glowing. Well, Steve, he's
glowing.
>> It's great. Yes. And then Boncharge
ships worldwide with easy returns and a
year-long warranty on all of their
products. So visit boncharge.com/diary
for 25% off on any product sitewide. But
you have to order through that link.
That's boncharge.com/diary
with code diary. Whether you are a
novice or you've been in the tax and
bookkeeping industry for years, if you
want to work with an experienced team of
professionals who are invested in your
learning and growth, there's a real
career opportunity with our sponsor
Intuit, the maker of TurboTax and
QuickBooks. Their self-paced training,
Intuit Academy, presents you with a
pathway to gain the necessary skills
that you'll need to feel confident
expanding your career within tax and
bookkeeping. And their team is extremely
supportive, too, with a large network of
experienced, credentialed professionals
right by your side as you learn and gain
experience. On top of all of this
upskilling, they also offer flexible
working schedules, whether that's
full-time, part-time, virtual, on-site,
or even letting you select your hours to
grow at the pace that you want to grow
at. Intuit's currently growing their
network of tax and bookkeeping
professionals. So, if you want to build
a career with them on your own terms,
just head to intuit.com/expert.
I'll put that on the screen. That's
intuit.com/expert.
How long does the average American spend
indoors? Does the average Brit spend
indoors? Good question. They're almost
identical. I think the Brits spend a
little bit more time outside than
Americans. The The last number for
Americans was 93%
and uh Brits is 92%.
>> Were we born to be outside? I think so.
You think our ancestors probably spent a
huge amount of time outside? Yeah. And
And And if you think about when I say
outside, that also brings into play a
number of other of the new start letters
that we haven't talked about. Uh
exercise. You're much more likely to do
good exercise outside. You're much more
likely to get air that's that's the
right type of air outside.
The other aspect about infrared light,
briefly,
is that trees
are highly reflective of infrared light.
In other words, if you're in an
environment where there are trees are
present, you're going to get much more
of this beneficial infrared light than
if you're in a concrete jungle.
So So So plants like this. In fact, the
way that we measure the deforestation of
the Amazon is through satellite imaging
that looks at infrared light because it
reflects infrared light back. So,
the best thing best situation to be in
is to be outside
on a green
on a day where where there's lots of
green trees. We've known for We've known
for decades that people who live in
green spaces
do much better in terms of diabetes, do
much better in terms of hypertension,
mortality, all of these things.
>> Depression. Depression, all of these
things, yeah.
And And when you think about this, um
you bring up a point in terms of of
correlation. How do we know it's not
depression? We used to say, "Well,
people who live in green spaces have
more money."
that people have They have more access
to things. Maybe that's what we're
saying.
I just have to tell you this study.
There was something called the
GreenHeart study in South Louisville,
Kentucky. They did an amazing thing.
They took this 4-square-mile area
in South Louisville, Kentucky, urbanized
area.
And they measured everybody's hs-CRP.
What is hs-CRP? Highly sensitive
C-reactive protein. It's a marker of
inflammation, and it's been correlated
to bad things like stroke and heart
attack. So, if you have high levels of
CRP, that's not good.
So, they measured every They measured
about 700 people.
And then they did something
extraordinary. They purchased 8,000
mature trees,
dug holes, and planted 8,000 trees into
4-square-mile area. And these are trees
with leaves on them.
2 years later, they come back and they
measure all 700 people in their study.
Repeat the hs-CRP.
Dropped by 13 to 20%, which correlated
to about a 10 to 15% reduction in
strokes.
These people didn't change their
socioeconomic status. They didn't
institute an exercise program. And so,
really, it kind of shoots in the heart
the idea that the advantage that we see
with green spaces has to do with
something else that we're not measuring.
I actually believe that we'll talk about
fresh air, too, that things like
these plants,
but much bigger. This is kind of like a
bonsai plant. But But trees outside,
they actually have a benefit. And what
they represent, again, is
these things that
don't leverage the other parts of your
body in the in terms of the chains uh
that make all of the chains bigger cuz
they're they're they're they're having a
benefit. But you can't get the benefit
of this if you're inside a house. So,
what should we do about this in terms of
how what changes should I make in my
life to capitalize on this? Um this is a
This brand here is called Bon Charge.
They do these Yeah. these red light
devices. They do like red light saunas,
blankets, um masks. They're actually a
sponsor of mine because I I started
wearing this and I think they they found
out. And I started wearing it because of
my girlfriend. Yeah. She was wearing it
every day and I got curious. And so, I
as I always do, I'm always super
skeptical. Sure. So, I went on online
and started looking at some of the
research. And I was shocked. Yeah.
>> It made no intuitive sense to me that a
red light mask or any like red light
device could have a profound like what I
see is a profound impact on my health.
Like I didn't believe it Yes.
>> to start with. Yes.
>> like woo-woo stuff to me. I I Yeah.
>> But I couldn't disprove it. Right. All
the studies, many of which you've
referenced, um supported that it was
having a profound impact. And as I said
on this podcast before, my girlfriend's
always right.
She's like always ahead of the curve and
always right. So, I started wearing her
mask and now I have my own from Bon
Charge.
>> Yeah. Ish. Do you recommend these kinds
of things? I I think it's reasonable to
do. I will say this. Um if you are
getting enough infrared light from the
sun,
what we find in studies, not
particularly with the mask, but we find
in other things, is that these these
other areas don't have as much efficacy.
It's almost to say, if you're on a ship
with a bunch of people with scurvy and
you already have a diet that's rich in
vegetables and fruits, eating an extra
lemon is not going to be that
beneficial. So, what do you do? Like a
lot of doctors do, we have shifts that
go from 7:00 a.m. to the p.m. So, you're
in the hospital, you're not going to get
outside. So, at lunch, I try to get
outside as much as I possibly can into
the sun for my 15 minutes.
>> What if you live in a cloudy country?
So, that's a good point. Uh clouds,
because they are water molecules, will
absorb a lot of the infrared lights. And
the problem is is that that's the
exactly the type of light that you want
to get. However, even on a cloudy day,
being outside, you're going to get more
infrared lights than if you were inside.
Okay, so I still get the light I need
when it's cloudy, but I just don't get a
lot.
Yes, exactly.
>> Is there anything I can do to get if
it's super cloudy and I know I'm going
to be indoors,
what do I do then? Yeah. So, the light
the type of lights that we have inside,
like these ones? Like these. Uh and and
and actually, I think the UK and the
United States are very similar in this
regard, is that we really can't get the
old incandescent bulbs. We're on LED or
or fluorescent. And if you think about
what they've done in terms of of these
bulbs,
the old incandescent bulbs used to give
you a very broad uh
spectrum. So, all the way from, you
know, just near blue all the way down
into the into the infrared. The way that
they've made the bulbs more efficient,
they said, "Hey, let's stop using energy
to give off this light that we can't see
and give a very narrow spectrum of light
that we can see."
So, think about what they've done. They
have for the first time in the history
of humanity,
they are now we are now being exposed to
light
in a very narrow spectrum without
anything else. Whatever in the history
of of humankind, when we light a candle,
when we would go outside into the
sunlight, when we would have a kerosene
lamp,
we were getting full spectrum.
In other words, we were never getting
blue lights without red lights. Now,
we're starting to get blue light without
red light.
So So do I change my bulbs?
It's difficult to do that because you
can't pick up in these incandescent
bulbs. Which brings me to I mean at
least at least in the United States, we
have laws now that outlaw the regular
selling of incandescent bulbs because of
energy efficiency. Oh yeah. I'm on
Google now and I've typed in
incandescent bulb. So there's something
called a general service lamp, which is
what the type of bulbs that you could
plug in. But if you decide that you want
to get a
bulb that you put into your microwave or
a bulb that you would do into a type of
chandelier that's a special type of
chandelier, those are still available.
You can still get incandescent bulbs for
those. What about these kinds of bulbs?
Is that an incandescent bulb? That's a
That is a That is an incandescent bulb.
Again, for these special type of lights,
but I'm I'm talking about the light like
the like the the good old fashioned A90,
I think it's called, light bulb that you
just screw in.
Those are
the 120 watts, those are getting more
difficult. You It's harder to find. You
can't go down to your Home Depot and and
find them there. So Glenn Jeffrey um and
this is this is a preprint that he is
he's done. He actually took
people
with that were working in this
environment with LED bulbs. He's
actually It's not peer-reviewed, it's
not published yet, but it's a preprint,
it's available on the internet, so I'm
not speaking out of class.
And what he did with 22 people is he
switched out
these LED bulbs and put in incandescent
bulbs.
And there was a there was a 25%
improvement in in color differentiation
in his study.
What does that mean? They were able to
distinguish colors 25% better than they
were when they were exposed to LED LED
When I say LED bulbs, these are the
bulbs that are high on the blue end.
Um so why would that be?
The retina, which is the back of your
eye, where in the light is coming in,
there's these cones that are
tremendously metabolically active.
They're constantly updating, sending
neural signals to the brain.
And there's It's the It's the one tissue
in your body with the most amount of
mitochondria. And it's because they have
to supply a lot of energy. As somebody
gets older,
that mitochondria is not producing the
same amount of energy. And so, the the
ability of the energy that those cones
have to draw on to do their work is
less. And so, they're not going to do
the job as well.
If you can perhaps increase the
the
the amount of output of energy from
those mitochondria, you could improve
the the the ability to visually
perceive. And and and
Glenn Jeffery has done this study
already, where he
for just 3 minutes,
670 nanometer light, very similar to
that mask, in the eye, only in the
morning,
improved
those people's ability to to to to
visualize and actually see.
And what does that mean for the broader
picture of our health?
>> would be able to distinguish colors
better and actually improve their
vision.
That's basically what it means.
Um and so, the question goes back to the
first question that you had at the very
beginning of the podcast, which is what
is the effect of low
energy output from the mitochondria.
Well, it depends on what tissue the
mitochondria is in. And so, if it's in
the eye,
then it's going to be a bit better
visual perception. If it's in the brain,
it's dementia. If it's You know, you see
You see what I'm saying? So, what we
start to see
is we start to see that a myriad of
different diseases are affected by the
sun.
I I challenge anyone to do this. If you
look at a publication in the United
States, I've seen it, where they map out
the amount of deaths
per in a calendar day.
Cardiac disease,
respiratory disease, kidney disease,
pneumonia,
all sorts of diseases, infectious
diseases, non-infectious diseases. You
will see a very clear pattern.
The maximum amount of deaths every year
occurs
within a month after the shortest day of
the year.
So, we're talking December, January.
We see the most amount of influenza
deaths at that time. We see the most
amount of cardiac deaths at that time.
We see the most amount of kidney deaths
at that time.
So, you might ask, well, that that's
because
that's because people get together at
Christmas time and they spread the germs
around more and we have Thanksgiving in
late November here in the United States
and and and and that's what's going on.
The problem is is if you look at
Australia,
which is on the other end. So, when is
their longest day of the year?
Their longest day of the year is in
December.
And that's when they have the least
amount of deaths, despite the fact that
they're all getting together for
Christmas in December. So, that doesn't
fly.
It's exactly the opposite. The most
amount of deaths occur in Australia, in
the Southern Hemisphere, in June to
July. That's their winter.
And so, what you see is deaths are
correlated to the length of the day.
This is the reason why whenever they
have to whenever they show you deaths in
the year, they always have to seasonally
adjust it. And the length of the day is
a proxy for the amount of sunlight.
>> Absolutely. You're much more you're much
more likely to get sunlight
on the longest day of the year than the
shortest day of the year, especially
when and and this is well known. There
there are some months, especially in
people who are doing shift work, like
7:00 a.m. to 7:00 p.m., there's
literally like December and January, you
will not see the sun because you are
going off to work before the the gets up
and you're you're coming home after the
sun is long set.
So, you're not you're not able to see
the sun, and so you could go literally
weeks
without seeing the sun at all.
Is there an optimal time of day to get
sunlight? Yes.
So, optimal time of day to get sunlight
would be for those that are concerned
about getting damage from ultraviolet
radiation. As we talked about, when the
sun is low in the sky, that's going to
be beneficial because the ultraviolet
cannot penetrate obliquely through the
atmosphere as well as long wavelength
radiation. So, when the sun is coming
up,
So, in the mornings? In the mornings,
and when the sun is going down in the
evenings. That's going to be the time
where you're going to get proportionally
more infrared light and
the least amount of ultraviolet light.
Now, when the sun is directly overhead
at noon, you're going to be getting the
most amount of infrared light at that
time, but you're also going to be
getting a lot of ultraviolet radiation.
And so, if you're not someone that's
gone out into the sun a lot, you may
want to avoid this period of time. Or,
as we talked about,
put on a broad-brimmed hat, put on
clothes. I mean, more clothes because
as we said, ultraviolet light does not
penetrate through clothes very well.
But, infrared light can. Does it matter
where the sun is hitting on my body?
Shouldn't. So, if I go outside and I'm
wearing a big hat, it's obviously going
to cover my eyes, my face, Yes. but
it'll be hitting my legs. For the
purposes of we're talking about with the
mitochondria, it will not matter.
However, if we're talking about
circadian rhythm, if we're talking about
getting circadian rhythm, that pathway
is through the eyes. So, you want to
maximize light through the eyes. Yeah,
so so this type of a light is called the
SAD light. So, your question had to do
with what part of the body does it need
to touch?
So, or need to be
touching. So, for the effect of the
mitochondria and and the metabolic
effects, it it should not matter, okay?
For this type of a light though, what
we're looking at is circadian rhythm.
And that's a that's a completely
different system that we're talking
about. That's not mitochondrial. That
has to do with the internal clock that's
in your brain that is regulating when
all of these things in your body
happens. And this light is about 10,000
lux. Lux is a way of measuring the
brightness of light. And what studies
have shown is that when you shine this
type of a light into your eyes, it had
it it's the way of of adjusting your
circadian rhythm. You don't have to If
you have a clock and it's not set to the
right time, there's a little thing at
the back that you can pull out and you
can change the time. Yeah. That pulling
out and and changing the time about when
things happen in your body is affected
most
by light. And light can actually shift
it one way or the other depending on
when you're shining that light. If
you're shining the light in the morning
time,
and this is what a lot of people do is
they'll use these these what they call
SAD lights. SAD stands for seasonal
affective disorder.
These lights, especially in the morning,
have a way of of not only setting your
circadian rhythm and making sure it's on
track, but also reducing depression.
There's a there's a portion of your
brain that receives light information.
It's called the perihabenular nucleus.
It's a long name, but it's it's it's
back there. And if it doesn't get
stimulated, it can cause depression.
And so so for people who live at high
latitudes,
uh further away, closer to the poles,
where the sun is getting up very late in
the morning, they're already off work
inside, this can actually be very
beneficial. So, what I would recommend
doing, you can pick these up pretty
cheaply on Amazon for about 20 bucks.
But they should generally be about 11 to
16 in from your face.
And uh what people should be getting is
about 3,000 lux hours.
Uh and what I mean by lux hours is you
multiply the lux times the amount of
hours that you're wearing it. So, 3,000
is where you ought to be. Because this
is 10,000 lux, you only have to look at
it for about a third of an hour or 20
minutes, and that should be enough. So,
is this a replacement for going outside?
It's a replacement for going outside
because of the fact that you're living
at a very high latitude and the sun is
not up, and because of the job that you
have,
it's going to uh it's going to have that
effect, but realize that this will not
replace the effect that the sun has on
your mitochondria. This is only to
affect the effect that lack of sunlight
has on depression. Okay. What if I'm
looking at the sun out of a window?
It depends on the window. So, you're not
still the window is going to be reducing
the amount of lux, so I would not
recommend if you can, I would not
recommend I would not say that staying
inside looking out the window is the
same as going outside. That's number
one. The other thing that you have to
understand is a lot of these windows,
especially if they're modern windows,
will be specifically designed to reduce
infrared light. I want you to give some
me any information you have yeah as it
relates to light health Yeah. that will
improve my life, things that I can act
actionably do tomorrow. Obviously, one
of them is that I'm going to go outside
and make sure I get some sunlight
ideally in the morning. Yes. We talked
about this sad lamp
for people especially that live in
certain countries which it which have
less sunlight
>> Correct. to set their circadian rhythm
and to help with things like mental
health. Is there anything else I should
be thinking about or can do or change?
Yes. So, just like we had in our
mnemonic of new start, rest and exercise
both at the same time and then yet the
short of opposite of each other, it's
important to have darkness.
Okay. It's important to have darkness,
and this is a real issue. This is one of
the biggest issues is the fact uh there
was a study that was published recently
and the title was dark days and bright
nights,
and that correlated with
uh increased mortality.
I mean, that's how most of us live.
That's the problem. We have dark days
and we have bright nights, and what we
really should be having is bright days
and dark nights. So, just as important
as it is to have bright sunlight and
getting outside in the middle of the
day, we also need to start working on
getting darker nights as well. And how
do we do that? Turning things off.
Uh getting the screens away from our
eyes. Um these are really important
because the screens have a lot of light
and the light what's going on here? This
is the reason why it's important.
There's two reasons actually. Is the
light that's going into our eyes is is
doing two things at night. Number one,
it is shutting down melatonin production
from the pineal gland. And as we just
talked about, melatonin's a very
powerful antioxidant that's very
beneficial.
The second thing that it's doing is it's
confusing your circadian rhythm. You
see, your circadian rhythm is designed
to see light as day.
If your If your eyes are seeing light,
your brain thinks it's the day. So, if
it's 10:00 at night and your eyes are
seeing light, your circadian rhythm is
saying, "I must have made a mistake. I
thought it was 10:00. It must not be
10:00 because look, there is light."
And so, what it's going to do is it's
going to adjust itself
and delay everything because it's
saying, "Well, it can't be 10:00 at
night. It must be 6:00."
And so, therefore, when you would
normally feel tired and sleepy at 10:00
at night,
after a number of days of doing this,
you're not going to feel sleepy until
1:00 in the morning.
These devices we have, they spit out a
lot of blue light, right?
>> Yes. Is there a way to like turn that
off? Yeah, actually a lot of these come
with uh with with tied to the clock
where after a certain time of night, it
will shift its its uh spectrum to a more
red spectrum. So, it's giving you less
blue light. The problem is is that while
the sensor in your eyes are tuned more
to blue light, it's not just blue light.
So, really the solution The best
solution is to turn off the lights.
The next best solution is to have more
of a red shift
or you know, put these glasses on at
night.
So, these are blue blockers. They're
trying to eliminate blue, but I'm I'm
still getting light in and that's enough
light to shut down melatonin production.
Even with those on?
>> Yeah. Absolutely. But you're telling me
these help? They're better than not
turning off the light.
And you're saying I still get light in
because there's light coming over the
top.
>> Even even that light there is still
going to bleed and it's going to bleed
into that part of the spectrum and cause
melatonin to be shut down. Yeah.
So, it's just the eyes are the sort of
the barometer for Correct.
>> what time of day it is.
>> Correct. And and the problem is is that
even when you close your lids,
light can still get through the lids.
What do you think of these sleep masks?
>> I think they're I think they're great
in terms of the fact that we now know
that closing your eyelids still can
allow some light to go in. So, if you're
in if you're sleeping in an environment
where, you know, light is out of your
control. If you're living in the city
and you can close your blinds but
there's still light that's coming in,
these things could actually be very
beneficial. I don't recommend
nightlights in bedrooms. You don't
recommend
>> not. I Even even clock radios or air
conditioners with LED displays on them.
That's that's just like total light
pollution to your bedroom. Your bedroom
should be as dark as possible. What if I
have those lamps that don't have blue
light in them?
Cuz I think my girlfriend puts some of
those by the bed. Yeah. Do they do
they still not great?
>> Again, the best thing is no light. The
second best thing is light with no blue
light in it and then the worst is, you
know, blue light.
What about candle light?
That's interesting.
Um there was a study that was done
where they compared someone reading at
night with a book with a light bulb
shining on it versus the LED, uh you
know, like a Kindle or whatever, okay?
What they found was that there was a lot
more light coming out of the Kindle than
there was just reading the book with the
with the lamp. And it and it delayed
sleep onset.
So Which delayed sleep onset? The
Kindle. The Kindle. Yeah. It delayed
sleep on enough to actually shut down
actually delay the circadian rhythm and
shut down melatonin production. So the
answer to your question is is candle
light's great. The only thing I'd be
concerned about is just the fire risk.
Yeah, cuz you fall asleep with that
thing.
>> Exactly. So the adjacent topic there was
vitamin D which we we touched on a
little bit. Do vitamin D supplements
work? Oh yeah, certainly. They do work.
I've tested them. Yeah, there's a number
of studies that have come out. Martineau
actually published in the British
Medical Journal. This is back
before 2020.
It was a meta-analysis of randomized
controlled trials showed that people who
supplement every day with vitamin D had
lower risks of acute chest syndrome.
The other one there was a recent study
that came out that showed that people
who supplemented with 2,000
international units a daily of vitamin D
had a lower risk of all cause autoimmune
conditions. We're talking rheumatoid
arthritis,
Crohn's disease, ulcerative colitis, you
name it.
That was that was a
study that came out that we actually
reviewed that on our on our Med Cram
channel. Cuz I've heard before in the
past that a lot of vitamin supplements
we take don't even get into our
bloodstream and into our bodies.
Yeah, so so vitamin D is very
interesting.
It is a supplement and it is a vitamin
but it's also a hormone.
Okay. It's it's it actually manipulates
um
DNA production. So it's it is quite
interesting. But these these are are
well described randomized controlled
trials. So if you're looking at the
autoimmune condition, this was actually
a study that was designed looking at
cardiac disease. They actually had two
arms, one with
omega fatty acids and and vitamin D and
they showed that in the vitamin D group,
there was a statistically reduction
statistically significant reduction in
autoimmune conditions.
I supplement with vitamin D. I just
Here's the
Here's the concern I have is if you are
going to supplement with vitamin D,
make sure that you get your levels
checked.
Why?
The reason is just because it is a
fat-soluble vitamin and it is possible
to take too much.
What happens if you take too much? It
can affect calcium metabolism and you
can have issues with calcium, too high
of levels of calcium.
It's very rare,
um but it can happen.
And I don't mean to say that in a sense
that I would I dissuade people from
supplementing because I think
supplementation can be good, but it at
some point you want to get a level
checked to see where you are. The other
reason is is because
based on your body habitus, based on
your skin color, because people with
darker skin, it's harder for them to
make their own vitamin D. They need to
be more time outside, especially if
they're at high latitudes. So, like me
living in the UK.
>> Exactly. I need to be outside more. It's
going to be harder for you to make as
much vitamin D as as somebody who for
instance if you were living at a lower
latitude or if you had lighter skin,
yeah. What is vitamin D doing in my
body? Ah, good question. Lots of things.
So, vitamin D if you were to look at the
the structure of vitamin D. Actually, I
actually did research on this
interestingly in college. I used to make
starting material for the graduate
students. It's It's a lipid-soluble
molecule and because it's lipid-soluble,
it's able to go right through into the
nucleus and actually go onto the DNA and
combine with proteins that actually
affects the transcription of your DNA.
So, in other words, depending on which
cell type we're talking about, it can
cause a lot of interesting changes. So,
it affects calcium metabolism. There's
vitamin D receptors on your immune
system.
So, uh it affects your immune system,
affects calcium metabolism, a whole host
of things. My team did some research and
found that approximately 1 billion
people globally have a vitamin D
deficiency. Not surprising.
>> 50% of the global population has
insufficient levels of vitamin D.
Absolutely.
Yeah.
Yeah, so the the issue is is that as the
world becomes more industrialized, as
the world becomes more well-off,
they're able to create dwellings and
they're able to air condition those
dwellings. And we, as human beings, tend
to avoid extremes. We don't like things
too hot, we don't like things too cold.
Well, I mean, let's face it, in our cars
we have something called climate
control. We can set the We can set the
temperature and that's what the
temperature is going to be. There is
this other implications which we can
talk about in terms of hydrotherapy,
perhaps, if we get to that. But, um the
issue is is we don't like those
extremes. We don't like going out into
the sun. And when we don't do that, we
we suffer the consequences. Is there a
way for me to get vitamin D without
supplementation and without going into
the sun? Yes. Yeah, it's in uh certain
foods as well. Mushrooms, for instance,
uh certain types of fish. They're um
they're they they have vitamin D in them
as well.
This is a strange question. But, do you
think our body knows
which foods we're deficient in?
And really what I'm saying there is
if I'm vitamin D deficient, do you think
there's a part of my body that knows
that I I need to eat mushrooms?
>> a good question.
>> makes me hungry for mushrooms. I don't
know about that particularly. I can say
this, though. In people who don't get
enough sleep,
we tend to have a predilection to eating
more carbohydrate-rich foods.
That one we do know. Okay. And and we
can and this is the reason why people
who
This is the reason why many scientists
believe that people who don't get enough
sleep tend to have food choices that
tend to put weight on.
Every single one of you watching this
right now has something to offer,
whether it's knowledge or skills or
experience, and that means you have
value. Stan Store, the platform I
co-own, who are one of the sponsors of
this podcast, turns your knowledge into
a business through one single click. You
can sell digital products, coaching,
communities, and you don't need any
coding experience, either. Just the
drive to start. This is a business I
really believe in, and already $300
million has been earned by creators, and
entrepreneurs just like you have the
potential to be on Stan Store. These are
people who didn't wait, who heard me
saying things like this, and instead of
procrastinating, started building, then
launched something, and now they're
getting paid to do it. Stan is
incredibly simple and incredibly easy,
and you can link it with a Shopify store
that you're already using if you want
to. I'm on it, and so is my girlfriend
and many of my team. So, if you want to
join, start by launching your own
business with a free 30-day trial. Visit
stevenbartlett.stan.store
and get yours set up within minutes.
Of these cards that we have left in
front of us from the New Start
framework,
which one are you compelled to talk
about next? Water.
Water. Yeah. Okay, so tell me what you
mean by water, cuz people will think,
"Yeah, I drink enough water." Well,
first of all, we I don't think we do
drink enough water, but
I what what everyone talks about, you
know, the internal use of water, and it
makes sense.
But, as I was talking about before, the
the external use of water can actually
be very impressive. And it has to do
with uh body temperature, and it has to
do with the immune system.
So, we'll talk about water, but let's
sort of set the framework for that
conversation.
Your immune system is broken up into two
into two types. There's the innate
immune system and the adaptive.
We've become very familiar with the
adaptive immune system during COVID,
because all the talk was about
antibodies and antigens, and the fact
that SARS-CoV-2 was mutating, and would
the vaccines that made antibodies
against them be uh still functional. All
of that, where we have like where we
literally have a key with a keyhole that
it fits into and turns the lock and
these antibodies and they fit, that's
all the adaptive immune system. It's
very important, but it completely
eliminates or or removes from discussion
the innate immune system. The innate
immune system is really the body's first
defense.
And what's happening there is there's
these cells that are circulating, cells
like monocytes and natural killer cells
and a number of other other cells which
scour the body always looking for
something that looks
foreign to it. And it can tell based on
the molecular patterns of these of these
invaders that they're not supposed to be
there and they should be eaten up.
The major effector of this innate immune
system is something called interferon.
Interferon is a very
important molecule in the body and it is
effective it is so effective
at preventing viral infections that just
about every single viral infection that
plagues the human body today has a
defense mechanism against interferon. It
is it is a prerequisite. There's no
self-respecting
virus that can think it it can infect a
human body without dealing with the
issue of interferon.
Period. Think about interferon
as the security guard at the bank. And
if you are want to rob a bank, you've
got to have a plan for how you're going
to deal with the security guard.
Otherwise, you're not getting the money.
Does that make sense? Yeah.
So, there was actually an article that
was published a couple of years ago
where they talked about this this battle
between interferon and emerging viruses
and what viruses are doing to try to get
around interferon.
You may recall that back in 2002, we had
an outbreak of something called SARS,
which especially was pretty bad in
China, but also in Canada. The reason
why we were able to secure that outbreak
was because that everybody who came down
with SARS
developed a fever.
And so it was easy to tell who those
people were,
and and we were able to hospitalize and
isolate them.
The issue with SARS-CoV-2, and indeed
many infections like the common cold, is
that you don't necessarily get a fever.
And
fever is really important. And you're
like, what does this have to do with
water? We're going to talk about this.
Interferon
production goes up with temperature.
And in fact, the body's
fever mechanism is one of the ways that
it tells the body that it needs to
increase interferon to deal with the
viral infection. Is that why you feel
hot? You feel hot You may actually feel
cold. And the reason why you may feel
cold and even have chills is because the
way you feel is a product of what your
temperature is and what your thermostat
in your body is set to. So, if your body
and your if your body's thermostat is
saying, "Okay, here we are at 98.6
or I guess in in terms of Celsius, 37°
and you develop an infection, the body's
going to say, "Whoa, we have an
infection and we need to increase the
body temperature. We're going from 37°
or 98.6 up to 38° or or 100.4."
Because your actual body temperature is
below where your body wants it to be,
you're going to feel cold. You're going
to shiver to try to increase that
temperature, so you go up with that.
Now, once the fever is done and the
infection is done
and it comes down, you're going to have
you're going to break a sweat. So,
that's that's why when someone Oh, he's
sweating. That means the fever is
breaking. That means your temperature is
coming down. So, you're typically you'll
feel cold, you'll feel like you're
shivering, you'll want to get into bed
and and and put the covers on, and
that's when your temperature goes up.
That and and that's for a reason.
Because what happens when the
temperature goes up in your body is that
creates an environment where the virus
that can't replicate very well. All
viruses really cannot replicate very
well at high temperatures, including
SARS-CoV-2. It's also a signal
to your body to produce more interferon.
So, there was a study that was published
last year where they looked in mice,
which by the way have the same body
temperature as we do, and they found
that there was like five different
regulatory proteins, all of which led to
one endpoint, and that was to produce
this thing called interferon.
All of them jumped in production when
your body went from
30
7° to 38°. That's basically right below
a fever,
right? So,
the point the take-home point that I got
from all of that was that we should not
really be treating fevers unless they're
so high that there's other complications
that could occur like, you know, uh
racing heart rates or or um or having
seizures. But, we do this all the time.
We treat fevers because it feel makes us
feel bad, and we think that by treating
the fever we'll feel better, but what
we're actually doing is we're we're
cutting the legs out from our immune
system because part of the immune system
response is to generate a fever, and the
and the fever generates interferon. Now,
I I don't want to overstate this, but
let's compare the innate immune system
to the adaptive immune system. The
adaptive immune system is pretty
specific for a particular variant of a
virus. And for a virus that mutates very
rapidly like SARS-CoV-2,
the immunization may be very good in
terms of binding,
but if that
that virus mutates,
that binding is going to be affected in
some way. It may not affect
hospitalization, but maybe in terms of
of preventing infection. Do you know you
understand what I'm saying? So, the
different variants, we had the alpha
variant, then we had the the delta
variant, then we had omicron, etc.
Those
are material changes for the adaptive
immune system.
For the innate immune system, for
interferon,
it doesn't matter.
Interferon is just as effective against
alpha as it was for delta as it would be
for omicron. So, so let's set this up
again.
Water.
We said that water has a very high
specific heat, which means that if I
apply hot water
onto the human body, it's able to
transfer heat. This is why people get
burned with boiling water.
We don't obviously want to burn anybody,
but if we're able to put them into a
sauna, if we're able to put them into a
spa, if we're able to use hot towels and
apply to the human body to heat up their
body to cause a sweat,
in other words, if we're able to induce
artificial fevers in patients who have
these infections,
there seems to be evidence that the
interferon response will be will be
better. Uh there was a study that was
done looking at lymphocytes and taking
them out of the human body and at
different temperatures, once it hit
about 38, 39°, there was off-the-charts
uh 10 10-fold increase in interferon,
which is exactly what you would want to
have. Now, how do I know that interferon
levels are so important in things like
COVID-19? Well, there was a study that
was done that showed that high levels of
interferon
correlated with more mild
uh
uh SARS-CoV-2 infections and that people
that had low interferon levels had very
severe COVID-19 infections. So, you're
suggesting that we should
be in the sauna more often? Yes, and
it's based on data
that is
has been well documented in in the
Finnish sauna
realm.
So, people who use sauna
four, five, six, seven times a week are
more likely to have less
uh death from cardiovascular disease
than people who use sauna once a week.
And and in Finland, once a week is kind
of the standard. And why do they say to
do hot and cold therapy together?
So, they would
I would argue that the reason why it has
been argued to do this, and this goes
back to uh a number of papers that have
been written back over 100 years ago, is
what you're doing when you're doing hot
for a long period of time, let's say 20
minutes in the sauna. And what you're
doing is you're heating up the body,
and uh and and the whole purpose of that
is to increase the body temperature.
What the What the cold at the end does
is it does two things, they believe. The
first thing that it does is it causes
vasoconstriction. So, you put a brief
amount of cold onto the body, it's going
to cause vasoconstriction superficially,
so that when you're done,
you're not going to lose as much heat
through those blood vessels. And so,
you're going to keep the core body
temperature higher for longer, which is
exactly what you want to do. The other
thing that cold water does, again, is
the vasoconstriction. When you It's well
known that when you take a cold shower,
your blood vessels constrict, and when
when you look at a blood vessel on end
in in a person who's living and
circulating, there are a number of white
blood cells that are latched on to the
inside surface of that blood vessel.
When that blood vessel contracts, a lot
of those white blood cells that were
stuck get kicked off into circulation,
and they go off, and they do whatever it
is that they're going to do. It's called
demargination. So, two things for cold
right at the end. Doesn't have to be
very long, maybe just a minute.
It causes uh actually to keep your body
temperature higher for longer,
ironically, and number two,
demargination.
So, that's water, which is the W. Um
of these,
which one do you want to pick next?
Which one do you find most compelling?
Let's talk about air.
Uh real briefly. So, we said that air is
not just the lack of toxins, but
actually benefits. So, first of all, we
want to have good oxygen. We want to get
rid of carbon dioxide, especially in
buildings when there's no ventilation.
That's not good. But, there's been
actually a number of studies looking at
plants and trees and the fact that they
can give off things like phytoncides.
What's that? These are are aromatic
compounds that the tree actually gives
off. And when we look to see the effect
of these compounds on the human body,
they're actually very beneficial. They
interact with our immune system and
elevate our immune system and actually
can make us more relaxed. There's a
There's a lot of data in the Japanese
literature on on this in the what they
call the hinoki cypress forests, where
they looked at um these CEOs.
There's a podcast about CEOs. There's
these CEOs in Japan, and they took them
from their their jobs and basically took
them up into the mountains of the hinoki
cypress and had them walk around, took
blood tests, and they found that the
natural killer cells, which are so
important in terms of immunity, were not
only increased in number, but they were
also the the um
the the enzymes within them that break
down diseases or viruses were also
increased.
So, when they brought them back down to
uh
the city in Japan, they put them up in
hotels, and they infused
some of these uh these chemicals, these
um naturally produced uh phytoncides,
they're called, and they had almost
exactly the same effects in in these uh
in these uh subjects.
So, you think plants and being out in
nature could actually be giving us much
more than just clean air. It's giving us
chemicals which help us fight disease.
>> Absolutely. So, so again, here's this
dichotomy, inside versus outside. What
do you get when you're outside? We've
already talked about exercise. We've
already talked about uh sunlight. And
now we're adding to it fresh air. Not
just the fact that you have uh
low pollutants, which is certainly very
important, but the fact that when you're
around green plants, when you're around
green trees, there could actually be a
benefit. By the way, the benefit that
they found lasted for about 7 days. So,
just going out one day a week um can
actually have that benefit.
I think a lot about carbon dioxide at
you cuz obviously cuz I I spend a lot of
time sat in the studio recording and um
this is our big LA studio, but uh
in the UK, it started in a really small
room and there wasn't air conditioning.
And obviously I sit here sometimes for
several hours with a guest and we're
recycling CO2 at that point. And then I
read a couple of studies that showed the
impact that would have on my cognitive
performance and
That's all true. We actually had on our
on our channel uh with uh Meg Cran, we
had Dr. Joseph Allen out of the Harvard
uh public school of health.
Um and he he showed us. I mean, he
literally uh had the the CO2 meter and
just by cracking the window uh just a
little bit allowed carbon dioxide to
escape and brought down those carbon
dioxide levels. So, very important,
absolutely.
And for people that work in offices or
you know, travel in hotel rooms or are
inside a lot, what should they be
thinking about and how can they go about
making sure that the air quality is
optimal?
Well, uh
the surrogate for that is carbon dioxide
as we mentioned. So, cracking open a
window if they're able to, if there's a
door that they can uh open up safely
without, you know, compromising
security. These are all things that uh
would be very very beneficial. Even
rolling down the window uh in in uh
in in car and and maybe taking making
sure that we're taking the uh that
recirculation button off when we're when
we're driving. I got friends that won't
won't stay in certain hotel rooms unless
the window opens cuz you know in a lot
of hotel rooms, especially ones that are
high up, you can't open the windows. And
there's also a bunch of devices that we
um
in our UK studio, which is smaller,
we found on Amazon for a you know, not
super expensive, that we just sometimes
put on the floor in the studio just to
see Yeah. how we're doing. I'll link
some of that stuff on screen if anyone's
interested in getting seeing what the uh
CO2 are in whatever room you're working
in. Yeah. What is uh what's next on your
list then here?
>> Well, we've talked about I mean,
exercise, nutrition, temperance, these
are things that a lot of people talk
about. Not many people talk about trust.
When you say trust, you really mean
religious faith and
>> Religious faith uh
something that would give you a a way of
of dealing with uh stress and and
anxiety. That's really where this comes
down. And there's been actually a number
of studies that have looked at that. So,
yeah, basically the Bible. Um or it
doesn't have to be the Bible as well.
There's there's other faith um
denominations that that look into this
as well. Number of studies that have
looked at trust in God and how that
relates
to anxiety. So, a number of studies have
shown that people who have a good
faith and trust in a God that is uh or
or in a religion that is supportive and
not non-supportive, they have less
anxiety, less depression, have a faith
community that they can uh engage with
and and be supportive.
Um and I think that that's that the
literature is uh where where as you have
it this the science behind that is not
as strict as it would be for like a
randomized placebo control trial.
There's a lot of associations that you
have to say here. Um that it certainly
is one of those pillars that I believe
helps with all of the those links. What
do you think's going on there? So, you
were telling me that from what the
literature's saying, people
>> who have a faith in a God Yes.
are insulated from depression and
anxiety in some interesting way. Yeah,
that that's a question that a lot of
people have tried to answer and and they
believe that it comes down to if you
have a trust in in a God that is looking
out for you
and is there on your side uh then that
type of relationship does lead is
associate let's say I shouldn't say does
lead to because that implies causation.
Let's say it's associated with
a reduction in depression, a reduction
in anxiety particularly.
Um there's there's an there are some uh
studies that have been done particularly
in uh in Christianity where there was a
study that was published. This is Krauss
and uh out of I believe University of
Texas where he did a survey and he asked
people
how they forgive.
And he he divi- he basically divided
them to two different groups. There were
people that would forgive give
conditionally and people that would
forgive unconditionally. Let me put it
into practical terms. Someone does
something to you.
And you say oh that's okay, I forgive
you.
The question is would you forgive that
There's some people that would only
forgive if that person came back and and
you know, did some sort of act of
contrition. Like okay, I'll forgive that
person they came back and apologized or
I'll forgive that person they came back
and they did you know, whatever it is.
That would be considered conditional
forgiveness.
The other type is unconditional
forgiveness. So in other words, someone
does something to you, you don't see
them again. Or or they've never
expressed any kind of you know, being
apologetic for what they did. They still
get forgiven. So that's unconditional
forgiveness.
What they found in the study when they
divided that is that the people
that forgave unconditionally
had less
depression.
They had less feelings of inadequacy.
They had less anxiety regarding uh end
of life. They had all They had all of
these They had more The people that
forgave conditionally
had more somatization of depression.
So, these were real medical
you know, things that they could
actually diagnose with surveys and and
and tests that are well validated. And
and what what would decide between these
two was how they forgave.
So,
they were puzzled by this. They said,
"Well, what Well, what then what
determines whether or not someone is
going to forgive conditionally versus
unconditionally?" So, they looked at a
bunch of factors and none of them stood
out except for one. And and the odds
ratio on this was like 2.5.
And and it boiled down to this one
question.
Do you believe
that God has forgiven you?
That was That was the major thing. If if
somebody believed that the God that they
had faith in had forgiven them, they
were two and a half times more likely
to to forgive somebody unconditionally.
Which then meant Which then was
associated with all of these other
things being low, like low less
depression, less anxiety.
So,
to me that that's an that's that's
fascinating that that in their minds
this is what's actually happening. And
so, there have been randomized
controlled trials where they have When
people are doing therapy, like let's you
say have you have anxiety. There is
cognitive behavioral therapy that we can
do for those people.
But, what has been shown in a randomized
placebo controlled fashion is that if
somebody is of a faith
and you inject into that cognitive
behavioral therapy aspects of that
faith,
the cognitive behavioral therapy is even
more effective.
So,
I guess I should preface this by saying
I don't believe that any of this stuff
should be placed on people without their
permission. So,
I'm working I work in a healthcare
environment. So,
do I go and pray for people
who don't believe? No. This is something
that that always has to be done
it has to be asked permission.
Do you think
>> Yeah.
people who believe in God are
healthier generally?
All other factors It would seem the data
would indicate that
people who
have a healthy relationship with their
church, who have a healthy relationship
in God, are associated with less
disease. Cuz from a causation point of
view, you could say well Causation,
yeah. So, this this is what we don't we
They probably have more friends. They
probably have Yeah. So, the question is
is whether or not people who are
healthier and have more friends are more
likely to be religious or is it the
other way around? And and sometimes it's
difficult to tell those things.
But I imagine there's a great calming
force that comes from believing in a
higher power.
Absolutely. And and the other thing that
the other thing that's interesting about
all of these like new start stuff is
when you look at other particular
religions,
how a lot of these things are actually
incorporate in this. Like for instance,
the Hindus are very famous for getting
up in the morning and welcoming the sun.
And we just talked about the benefits of
of sunlight. We didn't talk too much
about nutrition, but fasting is is an
important part of that and and and
Muslims are are obviously um
part of their religion is actually doing
fasting during Ramadan. So, religions
have a hot and cold practice as well,
don't they? Yes, yeah. At least through
history. And on the flip side of that, I
would say that it's also shown that if
you have a unhealthy relationship, like
if you have if you believe in a God who
is vindictive or who's out to get you or
who's going to do something to you
unless you do something else, that has
also been shown to be negatively
impactful.
So, it depends on the relationship that
you've got. What do you see in your
practice? Because you said something
earlier that you you're often there at
the end of people's lives. Yeah. Uh some
unfortunately sometimes I'm the last
person they see.
And and it's
you start to realize that you cannot I
mean that death is inevitable.
And all we do in medicine is delay the
inevitable.
So, what we try to do
and um and and I have a colleague uh
who's very philosophical about this is
we try to make sure that when these
things happen that they happen with
dignity and we celebrate the person's
life and and making sure that it's done
in the way that they would want to have
it done. What do people say as they're
about to die?
People become very
it's very different uh for for different
people, but uh they can become very
circumspect and and uh
I've seen such such contrasts. People
are ready to go. People feel like
they've they've done what they've come
to do. And uh they don't want anything
further to do. Like we're we're there to
to to to to to delay death, right? We're
there to put them on a ventilator or to
give them this medication. And you would
be surprised people who are look, you
know, relatively healthy, but and
something is happening that we could
easily correct. They're like, "No, I I
I don't want that. I I I choose not to
have that." And we have to respect
obviously what they
what they choose. Obviously, we have to
educate them to make sure that they're
making the right choice, but once once
they have given all the information
ultimately they're the one that makes
the decision. So, you see people choose
death.
When we can intervene in artificial
ways, they would rather not have that
and they would choose death, yes. Are
there any particular cases that changed
you?
Yeah.
Yeah, there's there's there's a case
that changed me. But not in the way that
we've just been talking about where it
was horrible. This is this is actually a
miracle.
I've actually seen a miracle happen. And
for me it happened early in my training.
So, it it it made me think twice about
being a prognosticating physician. A
prognosticating physician?
>> Yeah, saying oh
you're never going to walk again or or
you've only got 2 years to live. I I I
must have missed that day in med school.
I just didn't show up that day. This was
a young guy. He was he had he had
testicular cancer.
And he went to the operation. The
testicular cancer surgery was a success.
Unfortunately, during the operation
something happened. He didn't get enough
oxygen to the brain and he came out of
the operation with with anoxic injury of
the brain.
This guy must have been in his 20s. And
he had a young wife.
Um and uh
I had come onto the rotation as a as a
as a as a resident. And uh
we had attendings and you have to
realize in medicine you have attendings
above you and what they say is just, you
know, that's that's the word. That's
what happens and and the ICU attending
we were the ones that were sort of
taking care of the patient cuz he was on
a ventilator but there was the neuro
neurologist who looked at everything and
says, "Look, this guy is not waking up.
He has severe anoxic brain injury. We've
looked at the scans. This is what's
going to happen."
And so um
everyday we'd round on this guy and he
was just he was just a shaking mess. He
was just there and he was just kind of
shaking. His eyes were rolling. No
response. Nothing.
And everyday his wife would come in.
Young wife. And she uh
she just didn't believe that this guy
was going to be like this for the rest
of his life. He was going to wake up
eventually and so she he would she would
be at his bedside like attending to him
and making sure this that and the other.
And even asking us to put, you know,
some special concoction that she made at
home into his tube feeding so that this
could go and help him make him better.
And we would we would go along with her
but I was looking into my attendings and
they're like, "She's she does she
doesn't understand what's going on. She
doesn't understand that he's never going
to wake up."
So, this is this is what I'm seeing. Uh
one day she came in and she's and she
just had this
smile on her face. She was just uh so at
peace and a smile. And uh they they were
Hispanic couple, so we had to ask a
translator what was going on. And she
told us, she said, um
I had a dream last night.
I had a dream that he was going to come
home.
And she was convinced.
Just absolutely happy, beaming. And
we're like, man, this lady
is is crazy. She doesn't understand
what's going on.
Well,
days went on, weeks went on, and uh
one day uh and and where I was rounding,
it was it's just in this round nursing
The nursing station's in the middle, and
the doors to the rooms are all around in
a periphery.
And we were going around the circle
rounding on the patients, and I could
look in, and I saw him, and he was kind
of shaking, but he was kind of opening
his eyes.
And I said,
he seems to be focusing a little bit.
His eyes seem to be focusing a little
bit more than they would be.
And he kind of I I just said, I just
kind of put my hand up like this, and I
just kind of
and sure enough,
he put his hand up like this shaking.
And he put it back down again. I'm like,
what?
>> at you. Yeah.
What?
And I said,
let's go check this out again.
Long story short,
took months,
but that guy walked out of that
hospital.
6 months later, he and his wife came
back.
Walked onto the unit like like there was
nothing wrong with the guy.
And he gave us a big basket of flowers
to thank that unit for what they had
done for him. In my mind, I knew
that for most of that staff, for most of
that time,
they the people were just going through
the motions
keeping him alive, cuz that's what she
wanted.
Obviously, when when there were signs
that this guy was recovering, it was it
was complete shift. People were amazed.
And so, what that did to me in my career
was it made me think twice.
Like,
what why did this guy get better? Now,
he was 22, he was young. And And
typically, if something like that is
going to happen, it's going to happen in
someone who's very young, whose mind is
plastic, who can who can survive that
type of a situation.
But it really
it was a miracle.
I can't I can't say anything else. I
mean, it's not something that we would
know. All of the experts said that this
wasn't going to happen, but it happened.
What do you think happened?
I think he had a loving wife
who believed in him.
And something happened outside of the
physical and the mental.
Maybe the spiritual. I don't know.
It happens. It's very rare. And when it
does happen, it happens in young people.
That would be what the medical part of
my brain would say.
But the other part of my brain says,
"You know what? I only know about 10%,
maybe 5% of the world's knowl- No.
World's knowledge? 1% of the world's
knowledge. Maybe I have 5 to 10% of all
of the medical knowledge in this world.
And I would say probably the explanation
is somewhere in that other 80 to 90%
that I just don't know.
I think what it taught me was is that we
have to be humble
about what it is that we know.
There's things that we know we know, and
there's things that we don't know
that we don't know.
We talked a little bit about this
chemical earlier on, melatonin. Yeah. I
just wanted to close this off because I
had a question on it. Um a lot of people
take melatonin supplements
at night time to help them sleep. Yes.
Good, bad, and different?
I think it's good in certain situations.
So, if you're having difficulty falling
asleep, a little tiny dose of melatonin,
no more than 5 mg, can be actually very
beneficial. If you're wanting to shift
your circadian rhythm back instead of it
being pushed back, but you want it to be
advanced forward, melatonin can be very
beneficial. It's very beneficial for jet
lag. It's also beneficial for a few
sleep diseases, but I would not
recommend routinely for no other reason
taking large doses of melatonin. What's
the trade-off?
You said earlier on that everything has
side effects, right? And it impacts
another part of So, taking high doses of
melatonin can actually make you more
irritable.
And have irritable? Irritable, yeah.
>> In what regard? Just mentally irritable.
Yeah. What does that look like?
Things set you off,
um eat more easily. So, like a a mood
disorder?
>> Yeah, absolutely. Anything else with
melatonin that you're aware of?
Not that we have studies for. People
have concerns that sometimes taking too
much melatonin may actually affect the
melatonin secretion from the pineal
gland itself. I don't have evidence of
that as yet to see if that if that's
actually the case.
Dr. Rogers, is there anything else that
we haven't discussed that we should have
discussed?
We've discussed a lot.
Um
I think I think putting it all together
is
again, the links.
And if we have those links,
medications have their place, but the
way that they work is by breaking down
other parts of the chain to strengthen
the weak chain. That can have an effect,
especially at the end of life if you
want to sustain life. But if you're
interested in longevity, if you're
interested in making and living the best
life,
then you want to strengthen all of those
chains. And I believe the key to doing
that is something called NewStart.
We have a closing tradition on this
podcast where the last guest leaves a
question for the next guest not knowing
who they're leaving it for. And the
question that was left for you is what
is the area of your focus that you are
most dying to talk about which you are
almost never asked about?
This book, the Bible.
Uh which is my uh which is my tradition.
Evidence for
science
in the Bible.
What do you mean?
This we we what we've been talking about
is
the body
and the health of the body.
Um I'd like to put to to the test some
of the statements in the Bible to see if
they work scientifically.
Like turning water into wine?
No, well, potentially.
Uh that's a miracle.
What I was referring to is is this. And
this is what I've actually done and it's
actually quite interesting.
Is uh you know, Paul, who is one of the
New Testament writers in the Bible,
wrote to the Corinthians, "Don't you
don't you understand that your body
is the temple of the Holy Spirit?"
I said, "That's that's a really
interesting statement."
How would he come to that conclusion?
Like what does that mean, the temple of
the Holy Spirit? So,
the only temple at that time was the
temple in Jerusalem where they would
have the sacrifices and things. So, what
I did was I went back and this is and
this is answering the question is
I'm looking for evidence of scientific
truth
probably unknowingly
by some of the writers in the Bible to
see whether or not there is truth. Does
Does that make sense what I'm saying?
So,
if you look and most of Exodus 25
through 30
is this painstakingly detailed
description of the sanctuary that Moses
built in the wilderness that he
supposedly he got from God. This is what
he says.
So, here's a great way to see whether or
not this this all flashes out. Moses is
saying, "Here's the description of the
pattern that I got for the temple."
And Paul is saying,
"Your body is a temple." So, here's my
hypothesis.
If we look at the pattern in the temple,
should it match
the human body that they had no
understanding of at the time that Paul
wrote this. I We didn't know about cells
until Van Leeuwenhoek in the 1600s. We
didn't know about the circulation of the
heart
until the 1600s with um with
William Harvey, okay?
Yet,
if you look in the human body, you have
the blood system. You have blood
circulating around in the vascular
system. And then it And then it goes
into the interstitial fluid.
And then the interstitial fluid then
goes to the cell, which is There's a
There's a There's a plasma membrane on
the cell that you can't penetrate
through, but unless you actually have
the proteins to go. And then it goes
into the cell, which is a compartment
with two compartments within it, right?
You got the cell and the nucleus, right?
This is exactly the same structure that
Moses was given in in the wilderness.
And And by the way, uh Hindu temples are
actually similarly designed. They're
sort of this three-part situation. So,
you have this altar of sacrifice,
which is where the blood is.
That's That's the blood in the human
body. Next, you move to the laver,
which is this
container full of water.
And that's the interstitial space after
you go from the blood into the
interstitial space. Any pharmacologist
will know that this is the exactly the
pattern that you move to. The next thing
that comes is this structure
that has a veil that you can't penetrate
through unless you you go through it.
That's the cell cuz this this structure
is the building and it's got a room
within a room.
And that's exactly what the cell is. The
cell is this nucleus surrounded by the
cytoplasm. Well, in this room that you
go into it first,
there's pieces of furniture in there
that are very similar to the types of
organelles that you see in the in the in
the cytoplasm of the cell. For instance,
there's this seven-branch candlestick
that's in there that's burning olive oil
and producing energy. That's like beta
oxidation producing energy. That's
exactly what you see in the
mitochondria. But the final thing is you
move into the nucleus. And this temple
has something called the most holy place
where there's this altar of
where there's this ark of the covenant.
You've seen Indiana Jones, right?
>> Yeah. And and the first Raiders of the
Lost Ark, there's this ark and you open
it up and this is where the two tablets
of stone, the 10 Commandments, rested.
So, in
that area you have two tablets of stone
written by the hand of God
the code
of life.
And according to Jewish and and
Christian belief that this is the law
and if you break the law that's how sin
is and the consequences of sin is
disease and death.
Well, when we get to the nucleus of the
human body
you have two strands of DNA.
And on the strands of DNA is the code.
The nucleotides of which is the code of
life. If you manipulate that code that
leads to mutations which leads to
disease and death.
None of this was known until 1950 when
they discovered DNA. And yet
we have Paul
who's making this jump and saying your
body is the temple of the Holy Spirit.
I just I just find that fascinating.
Nobody ever asked me about that. But
that's what As soon as you ask that
question, that's the first thing that
By the way, there's so many other places
in in in the scriptures where I see that
alluded to. Um
it's fascinating. Paul Paul talks about
the body of Christ and how it's
one body, but it's made up of parts.
There's the hand, the foot. He didn't
know about cells, but that's exactly
what the human body is. The human body
is one body made up of many parts. Van
Leeuwenhoek didn't discover that until
the 1600s. We didn't have cell theory
until the 1800s.
So, this is it's interesting to me how
statements are made in ancient texts
which have scientific relevance far
below the surface.
I just find that interesting.
Thank you so much and I hope to speak to
you again very, very soon. And thank you
for all the work you're doing because
you've made some of these difficult
scientific subjects so unbelievably
accessible. You have a real art for
simplifying.
And simplifying in a way that means that
millions of people you've got millions
of subscribers on your YouTube channel.
Millions of people can access this
information which is often confined
within the walls of some academic study.
So, thank you for the work you're doing
because it's going to it's I'm sure it's
already had a profound impact on many,
many millions of people's lives and I'm
sure my audience are deeply
appreciative. So, thank you so much
Roger. I appreciate you. Thank you
Steven. Thank you for having me on and
having this opportunity.
Make sure you keep what I'm about to say
to yourself. I'm inviting 10,000 of you
to come even deeper into the Diary of a
CEO. Welcome to my inner circle. This is
a brand new private community that I'm
launching to the world. We have so many
incredible things that happen that you
are never shown. We have the briefs that
are on my iPad when I'm recording the
conversation. We have clips we've never
released. We have behind-the-scenes
conversations with the guest and also
the episodes that we've never, ever
released and so much more. In the circle
you'll have direct access to me. You can
tell us what you want this show to be,
who you want us to interview and the
types of conversations you would love us
to have. But, remember for now we're
only inviting the first 10,000 people
that join before it closes. So, if you
want to join our private closed
community, head to the link in the
description below or go to
doacircle.com.
I will speak to you there.
I see messages all the time in the
comment section that some of you didn't
realize you didn't subscribe. So, if you
could do me a favor and double-check if
you're a subscriber to this channel,
that would be tremendously appreciated.
It's the simple, it's the free thing
that anybody that watches this show
frequently can do to help us here to
keep everything going in this show in
the trajectory it's on. So, please do
double check if you subscribed and uh
thank you so much because in a strange
way you are you're part of our history
and you're on this journey with us and I
appreciate you for that. So, yeah, thank
you.
Interactive Summary
Ask follow-up questions or revisit key timestamps.
Dr. Roger Seholt, a critical care physician, outlines eight pillars of health (NEWSTART: Nutrition, Exercise, Water, Sunlight, Temperance, Air, Rest, and Trust) that can strengthen organ systems and prevent chronic diseases. He emphasizes the importance of sunlight for mitochondrial health, explaining how infrared light penetrates deep into the body to support cellular energy production through melatonin regulation, contrasting this with simple Vitamin D supplementation. He further discusses how lifestyle interventions like saunas, time in nature, and managing sleep environments contribute to overall well-being and immune system resilience.
Suggested questions
4 ready-made promptsRecently Distilled
Videos recently processed by our community
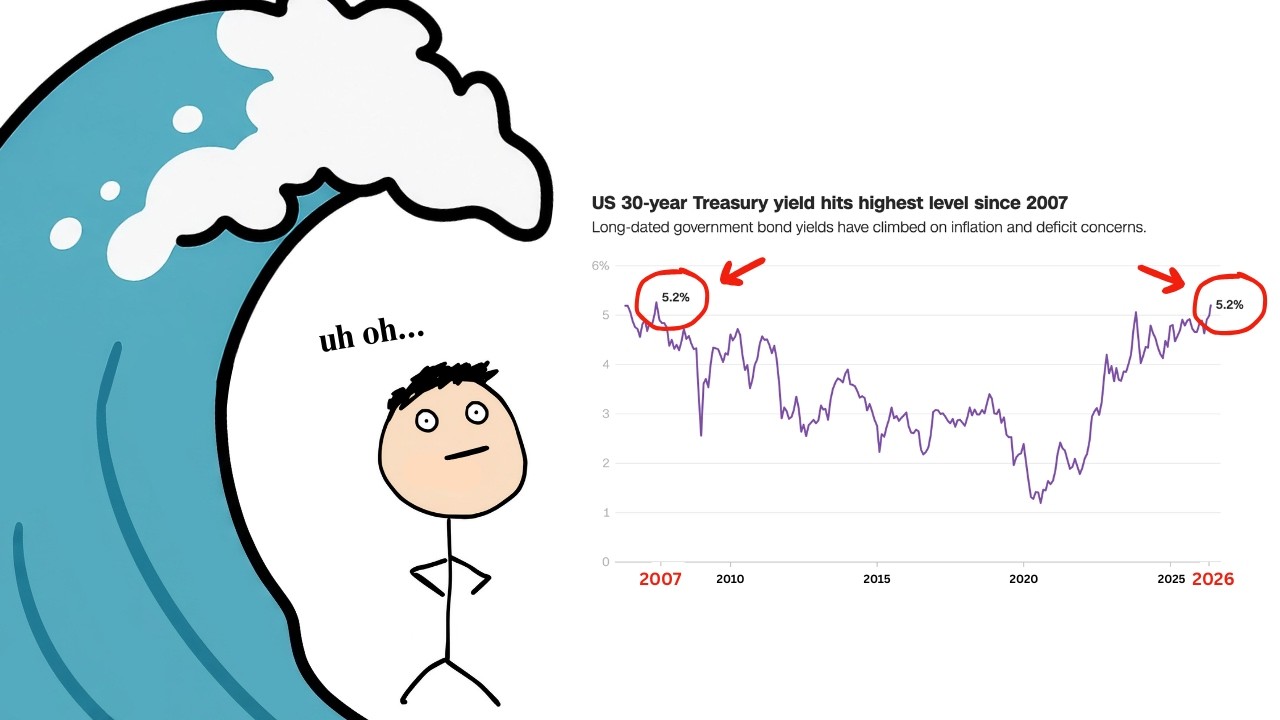
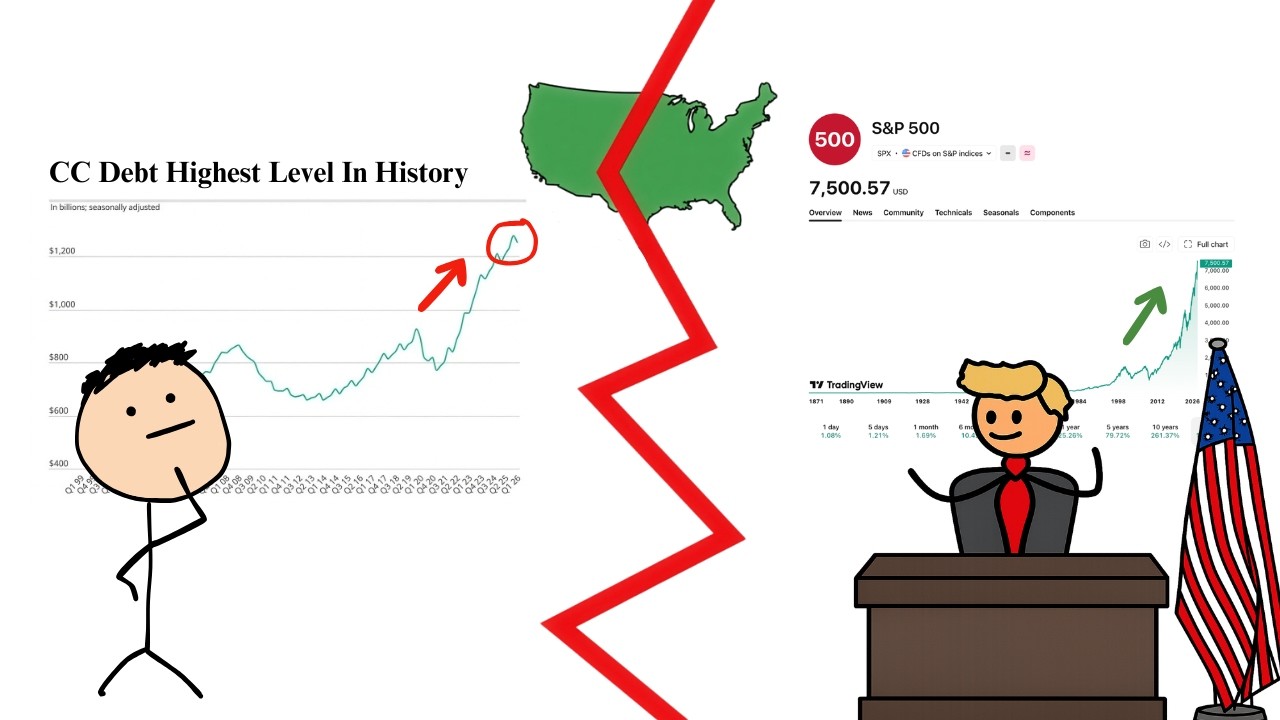

![[1hr Talk] Intro to Large Language Models](https://img.youtube.com/vi/zjkBMFhNj_g/maxresdefault.jpg)